CARDIOVASCULAR JOURNAL OF AFRICA • Vol 23, No 2, March 2012
e2
AFRICA
Discussion
Coronary artery fistulae are defined as abnormal communica-
tion between a coronary artery and a cardiac chamber or major
vessel, such as the vena cava, right or left ventricle, pulmonary
vein, or pulmonary artery. Fistulae arise from the right coronary
artery or their branches in about half the cases, and drainage
generally occurs into the right ventricle, right atrium and pulmo-
nary arteries. Coronary cameral fistulae terminating in the left
ventricle are uncommon.
1
Although the actual incidence of
congenital coronary artery fistulae is unknown, it was reported
to be 0.13 (0.8%) cases in an early study of 14 708 patients who
underwent coronary angiography.
2
Small fistulae usually do not cause any haemodynamic
compromise. However, large or small multiple fistulae can cause
myocardial ischaemia. Coronary cameral fistulae may present
with symptoms related to volume overload, and those drain-
ing into the left ventricle may show physiology similar to that
of aortic insufficiency. The mechanism of ischaemia is likely
to involve a steal phenomenon, with blood following the low-
pressure route to the left ventricle.
3
In a review of 363 cases of coronary artery fistulae, only 5%
of the fistulae were found to arise from both coronary arteries.
4
Bi-arterial fistulisation to the left ventricle is rare and only a few
case reports are presented in the literature.
5
Large coronary cameral fistulae have a variable natural
history. A small number of cases may undergo spontaneous
closure. In the remaining patients, indication for closure includes
increasing right-to-left shunts, left or right ventricular overload,
myocardial ischaemia, congestive cardiac failure and prevention
of endocarditis. The treatment options for closure of large fistu-
lae are surgical or catheter occlusion techniques.
Because of the multiplicity and small calibre of the fistulae,
neither treatment options were considered feasible in our case.
The patient’s effort angina decreased with medical therapy
during follow up.
Conclusion
Our case is unique because of its angiographic appearance.
Multiple fistulae homogeneously filled the left ventricular cavity
and this simulated left ventriculography.
We thank Prof Ismet Dindar for his continued support.
References
1.
Luo L, Kebede S, Wu S, Stouffer GA. Coronary artery fistulae.
Am J
Med Sci
2006;
332
: 79–84.
2.
Gillebert C, van Hoof R, van de Werf F, Piessens J, De Geest U.
Coronary artery fistulas in an adult population.
Eur Heart J
1986;
7
:
437–443.
3.
Sambu N, Sharma R, Kalra PR. Multiple coronary to left ventricular
fistulae.
Eur J Echocardiogr
2009;
10
: 352.
4.
Levin DC, Fellows KE, Abrams HL. Hemodynamically significant
primary anomalies of the coronary arteries. Angiographic aspects.
Circulation
1978;
58
: 25–34.
5.
Black IW, Loo CK, Allan RM. Multiple coronary artery-left ventricu-
lar fistulae: clinical, angiographic and pathologic findings.
Cathet
Cardiovasc Diagn
1991;
23
: 133–135.
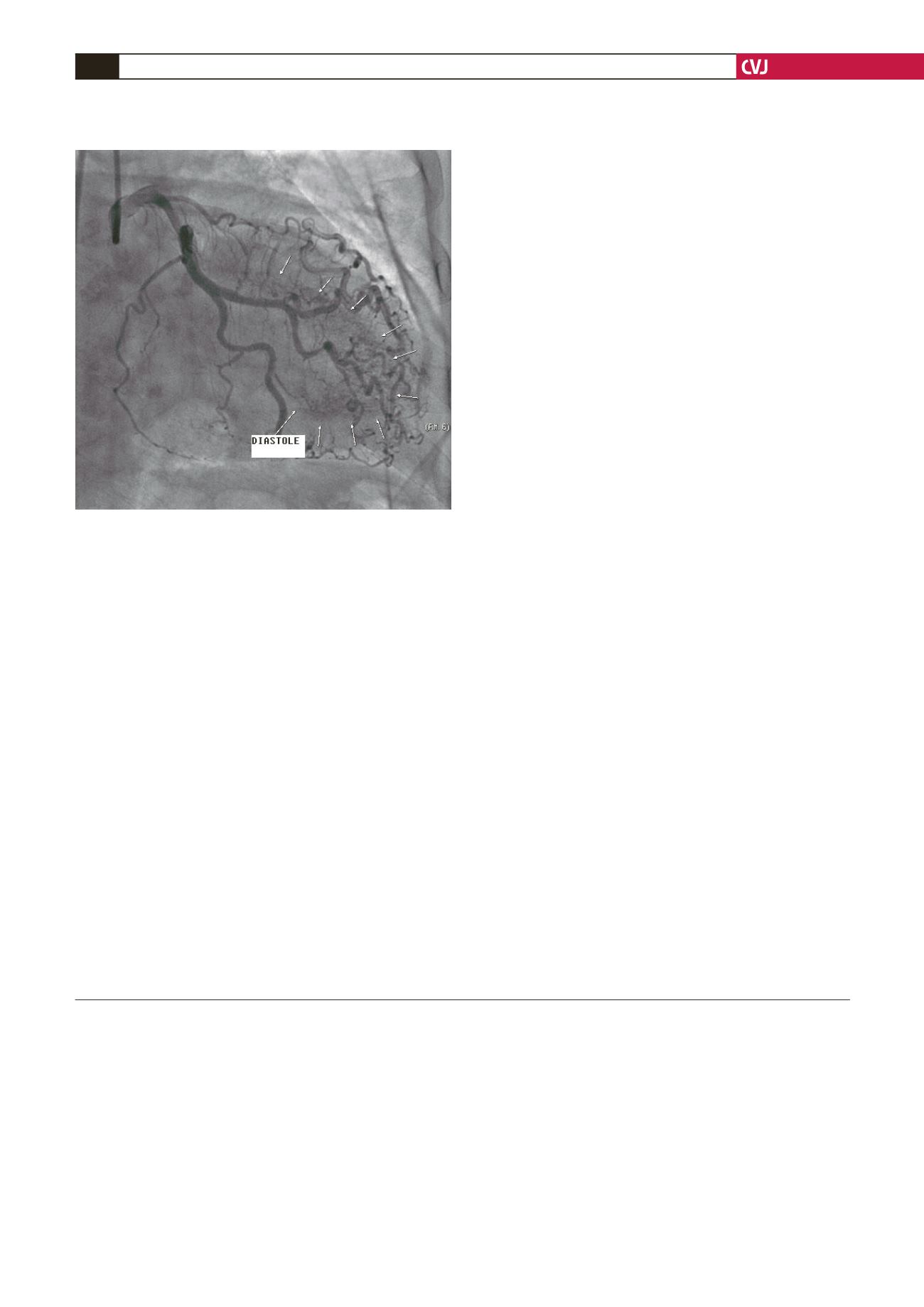
Fig. 3. Right anterior oblique view shows opacification of
the left ventricle by fistulae in diastole.


