CARDIOVASCULAR JOURNAL OF AFRICA • Vol 23, No 7, August 2012
AFRICA
e5
Discussion
To the best of our knowledge, this is the first confirmed case
report of PAH associated with HIV in pregnancy in Africa.
PAH has been reported in approximately 1/200 patients infected
with HIV, compared to a prevalence of 1/200 000 in the
general population.
1,2
The typical histopathological findings in
HIV-associated PAH are plexogenic pulmonary arteriopathy,
thrombotic pulmonary arteriopathy and pulmonary veno-
occlusive disease.
3
Pulmonary vessel endothelial cell proliferation and
vasoconstriction triggered by pleomorphic cytokines (e.g.
endothelin-1, interleukin-6 and tumour necrosis factor-
α
)
released by HIV-infected pulmonary macrophages and dendritic
cells are thought to play a central role in the pathogenesis
of HIV-associated PAH, which has no apparent association
with CD
4
cell count or viral load.
3,4
There is also evidence
that individual antiretroviral drugs (i.e. ritonavir, indinavir,
lamivudine, didanosine, abacavir and zidovudine) and a
combination of three drugs (indinavir, didanosine and stavudine)
at their therapeutic plasma concentrations may cause endothelial
dysfunction through endothelial nitric oxide synthase down-
regulation and superoxide anion production in porcine pulmonary
artery rings and human pulmonary artery endothelial cells.
5
It is
therefore possible that both the HIV infection and treatment with
zidovudine may have contributed to the pathogenesis of PAH in
this patient.
Clinical symptoms of HIV-associated PAH are dyspnoea, dry
cough, angina, near syncope or syncope and oedema. Clinical
signs are those of pulmonary hypertension and right heart failure.
The haemodynamic stress of pregnancy, labour, delivery and the
postpartum period are known to be potentially devastating in
patients with PAH in general, resulting in a maternal mortality
of 30–50%, despite modern treatment modalities.
6
The majority
of maternal deaths in PAH patients occur either during labour
and delivery or within one month postpartum. Cardiovascular
collapse is attributed to a mismatch between the physiological
limitations of PAH and the changes that occur with pregnancy
and delivery.
6
To the best of our knowledge, there are no outcome
studies in patients with the triad of pregnancy, PAH and HIV
infection.
While there are a number of treatment options for PAH
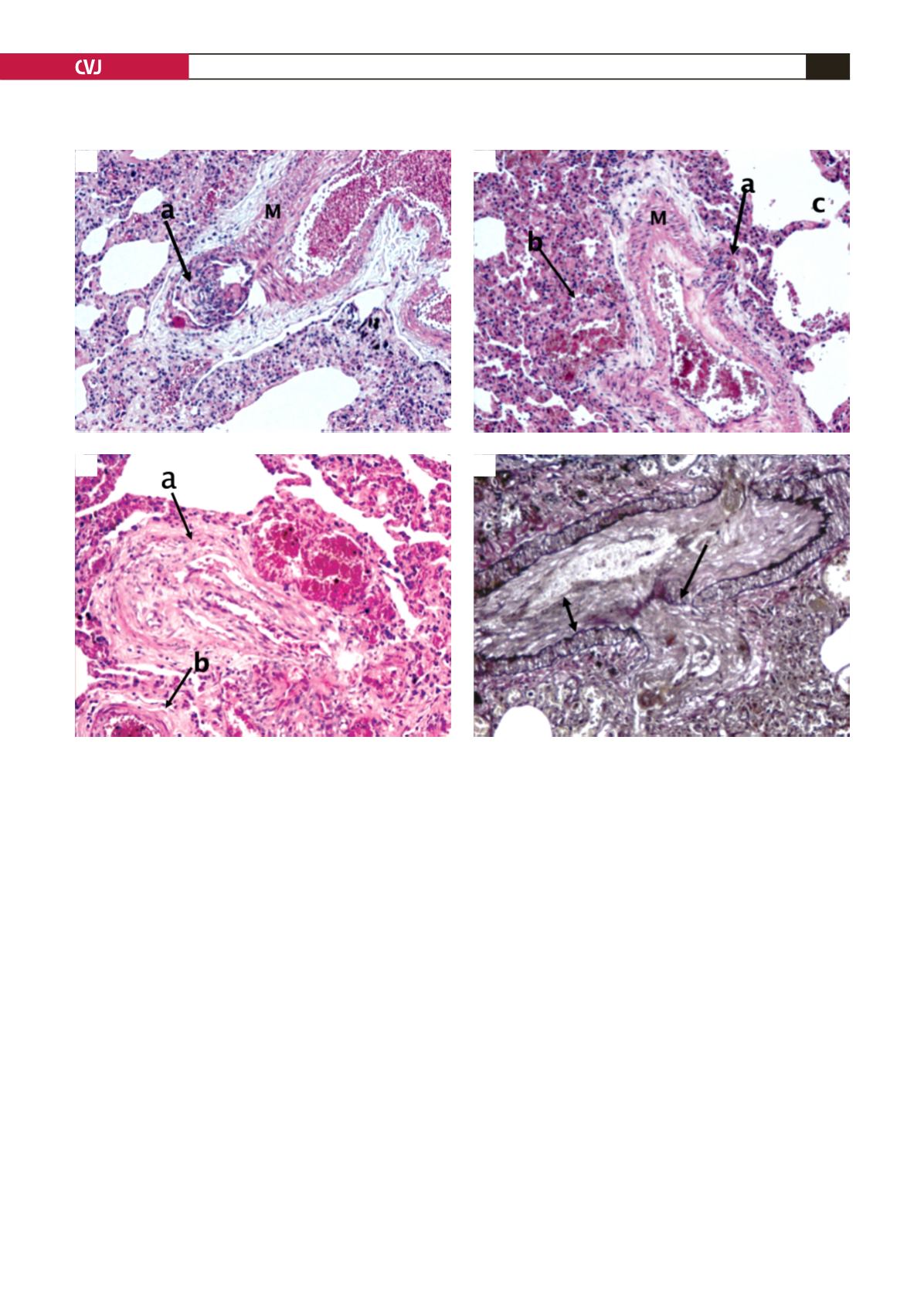
Fig. 2. A: A plexogenic lesion arising from a larger artery (a). The artery is characterised by a thick muscular coat and
association with a bronchus is not seen in this picture (M – media). B: A plexogenic lesion arising from an artery (a).
An abnormal thin-walled vessel adjacent to the artery (b). Alveolar spaces (c). C: A plexiform lesion showing a collec-
tion of thin-walled vessels (a). The edge of an artery (b). Congested alveolar spaces (c). D: Verhoef elastic van Gieson
(VEVG): note the deficient internal elastic lamina and fibro-intimal proliferation (double arrow).
A
C
B
D


