
















 12 / 74
12 / 74

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 28, No 5, September/October 2017
286
AFRICA
Methods
Rwanda is a small central African nation of approximately 12
million inhabitants (2013 estimate). The population is relatively
young and predominantly rural. The capital city, Kigali, with
a population exceeding one million people, is the location of
major medical facilities. Other medical facilities such as health
centres and hospitals are located at the provincial, district and
sector levels.
The Gasabo district, adjacent to the city of Kigali, has a
population of approximately 400 000 including its own urban,
suburban and rural areas. Data (2011) from the Gasabo District
Education Department indicated that there were 106 schools
with 67 538 registered primary and 8 989 registered secondary
school students.
Rwandan schools are classified by the Rwanda Education
Department as rural, peri-urban public and urban private,
according to their geographic location and to the socio-economic
level of the adjacent population. The majority of schools are in
rural areas and are considered ‘economically disadvantaged’.
The included population, for the most part, lived in sub-standard
housing without running water or electricity.
The sample size calculated for the study was 2 940, assuming
a prevalence of definite RHD at 1% in school-aged children
(6–16 years), with a precision of 0.4% and an inter-cluster
correlation coefficient equal to 0.001. When considering 2%
non-respondents, the final sample size was increased to 3 000.
Ten schools from the Gasabo district were selected for this
study using a stratified two-stage cluster sampling, where the
primary sampling units were schools from the three following
areas with different socio-economic levels: rural public schools,
middle class and urban private schools.
A second stage of preparation was based on individuals,
including all classes in each school where all school children were
stratified by grade, class and gender to ensure an equal number
of boys and girls from the grades included in the sample. Using
official lists of students, children were then randomly selected,
using the function RANDBETWEEN (Excel software).
The majority of students in five of these 10 schools were
classified by the Education Department as being economically
disadvantaged. From each of the 10 selected schools, a stratified,
randomised selection of 300 students was performed. Random
selection of an additional 50 to 100 students from each school
was also performed to constitute a reserve list. The original
group of 3 000 subjects included those from rural, peri-urban
and urban areas of the Gasabo district (Fig. 1).
Informed parental consent, subjects’ assent (if older than eight
years), and a questionnaire that included socio-demographic
data, as well as personal and family health histories were
obtained for each selected subject and alternate subject.
The study protocol was approved by the Rwanda National
Ethics Committee and the Rwandan Ministries of Health and
of Education. Socio-economic status was classified as high,
medium and low according to Gasabo District Education
Department criteria.
Educational sessions and materials about RF/RHD and
the programme’s objectives were developed and distributed to
school teachers, headmasters, administrators and parents of the
subjects representing the selected schools. Included were didactic
pamphlets, posters and banners in Kinyarwanda, the principal
language spoken by most Rwandans.
Echocardiographic screening procedures
The echocardiographic examinations were performed during
a 10-day period by 14 experienced US-certified sonographers
who were trained and followed the 2012 WHF criteria for the
echocardiographic diagnosis of RHD
10
(Fig. 1, Table 1). All
the sonographers held a certification by either the American
Registry of Diagnostic Medical Sonography (ARDMS) or
Cardiovascular Credentialing International (CCI). Additionally,
the mean number of years of experience exceeded 14 for the
sonographers.
The echocardiographic instruments, along with appropriate-
sized multi-Hertz, phased-array transducers, included: 11 SonoSite
(five Micromaxx + five Turbo + one Nanomaxx – all SonoSite
Inc, Bothell, Washington), one Philips CX50 (Philips Ultrasound,
Bothell, Washington), one Acuson Cypress (Siemens, Mountain
View, California) and one GE Vivid i (GE Medical Systems,
Milwaukee, Wisconsin).
Transthoracic echocardiographic examinations were
conducted in specially prepared rooms at each school. The
following views were obtained from each subject: parasternal
long-axis view, parasternal short-axis views, apical three- and
four-chamber views, along with colour-flow Doppler and
spectral Doppler interrogation of the intracardiac valves.
Two paediatric cardiologists were present during the
echocardiographic screening examinations. During or following
each echocardiographic examination, the sonographer and
paediatric cardiologist preliminarily discussed any findings of
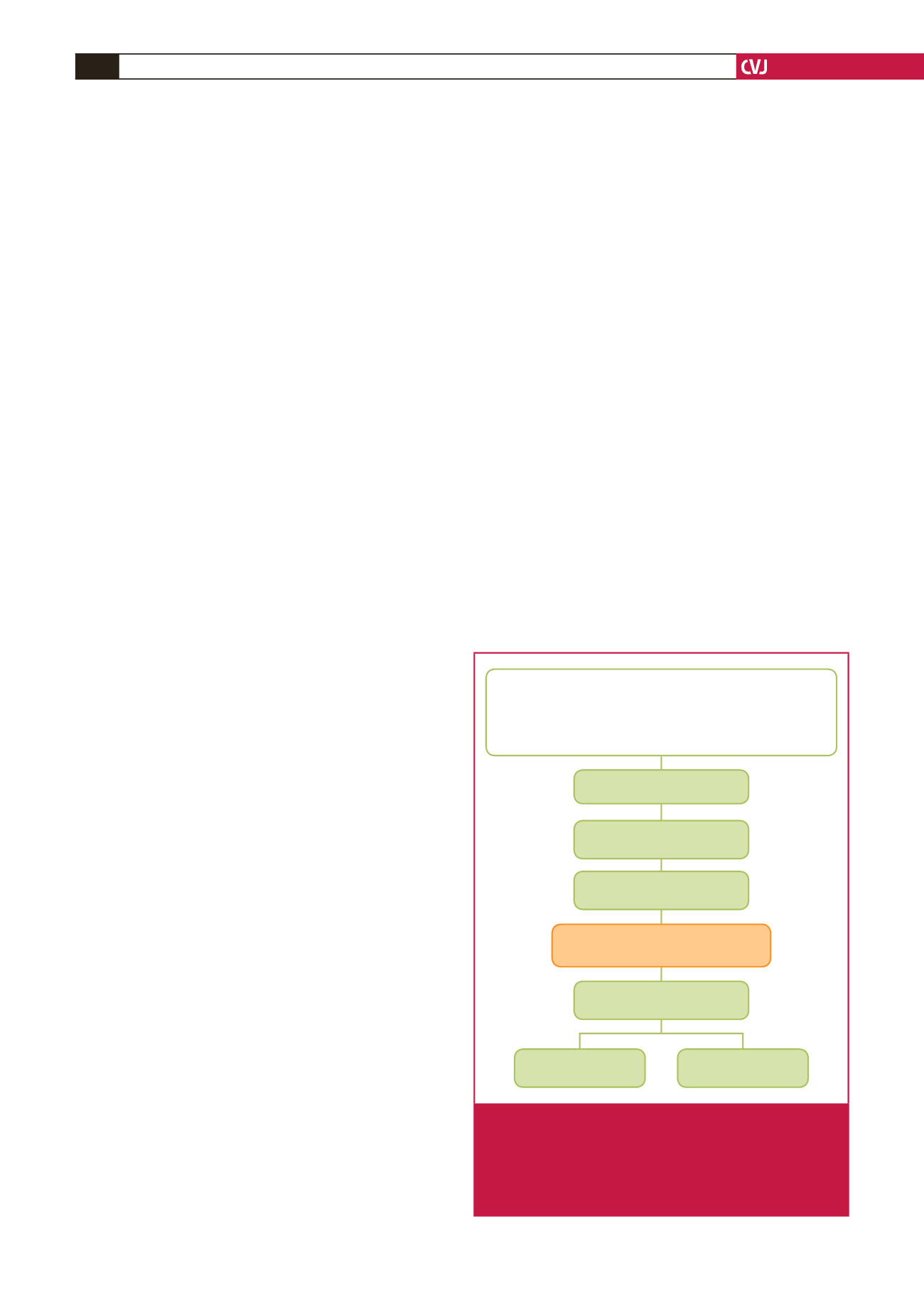
• Gazabo District: 67 538 primary school students; 8 989 secondary
school students
• Age: 6–16 years
• Sites: 10 representative schools: rural, peri-urban, urban –
300 children per school
• Sampling method: stratified randomised
Definite RHD
n
=
4 (0.16%)
Borderline RHD
n
=
13 (0.52%)
Children randomised
n
=
3 000 (100%)
Children selected
n
=
2 693 (90%)
Children screened
n
=
2 501 (83%)
RHD cases
n
=
17 (0.68%)
WHF 2012 echocardiography criteria:
definite or borderline RHD
Fig. 1.
Summary of methodology and echocardiographic
screening outcomes of the representative sample of
Rwandan school children in the Gazabo district of
the Rwandan capital, Kigali, and cases assessed as
definite or borderline rheumatic heart disease (RHD)
using the WHF 2012 criteria.
9