CARDIOVASCULAR JOURNAL OF AFRICA • Vol 22, No 2, March/April 2011
96
AFRICA
Secondary intracardiac Burkitt-like lymphoma in the
absence of HIV infection
AO MOCUMBI, L PAUL, L MACIEL, P SILVA, MB FERREIRA
Summary
Malignant lymphoma can involve the cardiac cavity or
myocardium as a mass. Since clinical symptoms of its cardiac
involvement are usually absent or non-specific, they may
be undetected during life. Burkitt-like lymphoma (BLL)
is a highly aggressive B-cell lymphoma with a high prolif-
erative rate. Histopathological characteristics are considered
borderline between those of classic Burkitt lymphoma and
diffuse large B-cell lymphoma. Extensive cardiac involve-
ment of BLL is rare and poorly documented in the literature.
We report the case of a child with BLL, presenting with
extensive infiltration of the heart in the absence of HIV
infection, and with right-sided heart failure and positional
dyspnoea as the major clinical problems. We highlight the
challenges for diagnosis and adequate treatment in poor
settings like ours.
Submitted 13/8/09, accepted 10/3/10
Cardiovasc J Afr
2010;
21
: 96–97
Secondary cardiac involvement of malignant lymphoma is not
uncommon, being observed in up to 25% of autopsy cases.
1
However, since clinical symptoms of this cardiac involvement
are usually absent or non-specific, these tumours frequently
remain undetected before death.
We report on a child who had Burkitt-like lymphoma (BLL),
presenting with right-sided heart failure and positional dyspnoea
as the major clinical problems.
Case report
A nine-year-old boy from a poor, remote, rural area of
Mozambique was referred to our hospital with a 12-month histo-
ry of thoracic pain, palpitations, shortness of breath, cough and
progressive postural dyspnoea. Dyspnoea was increased in dorsal
and lateral decubitus. The patient had been unsuccessfully treat-
ed with diuretics in a community health centre for nine weeks.
Due to progressive deterioration of his general and nutritional
status, and to the development of progressive upper thorax, neck
and facial oedema, he had been admitted to a peripheral hospital
for another three weeks before being transferred to our unit.
On arrival, the patient was in NYHA class IV. On physi-
cal examination he was fully conscious with dyspnoea that
was aggravated in certain positions, asymmetrical facial and
neck oedema, increased jugular venous pressure and cervical
lymphadenopathy. The vital signs were: pulse rate 116 beats/min,
temperature 38.5ºC, respiratory rate 24/min and blood pressure
100/70 mmHg. On cardiac auscultation a diastolic rumbling
murmur could be heard in the tricuspid area, and the auscultation
of the lungs revealed scarce rales. The abdomen was distended
with considerable hepatomegaly, splenomegaly and ascites, and
there was incipient oedema of the lower limbs.
The electrocardiogram showed normal sinus rhythm with no
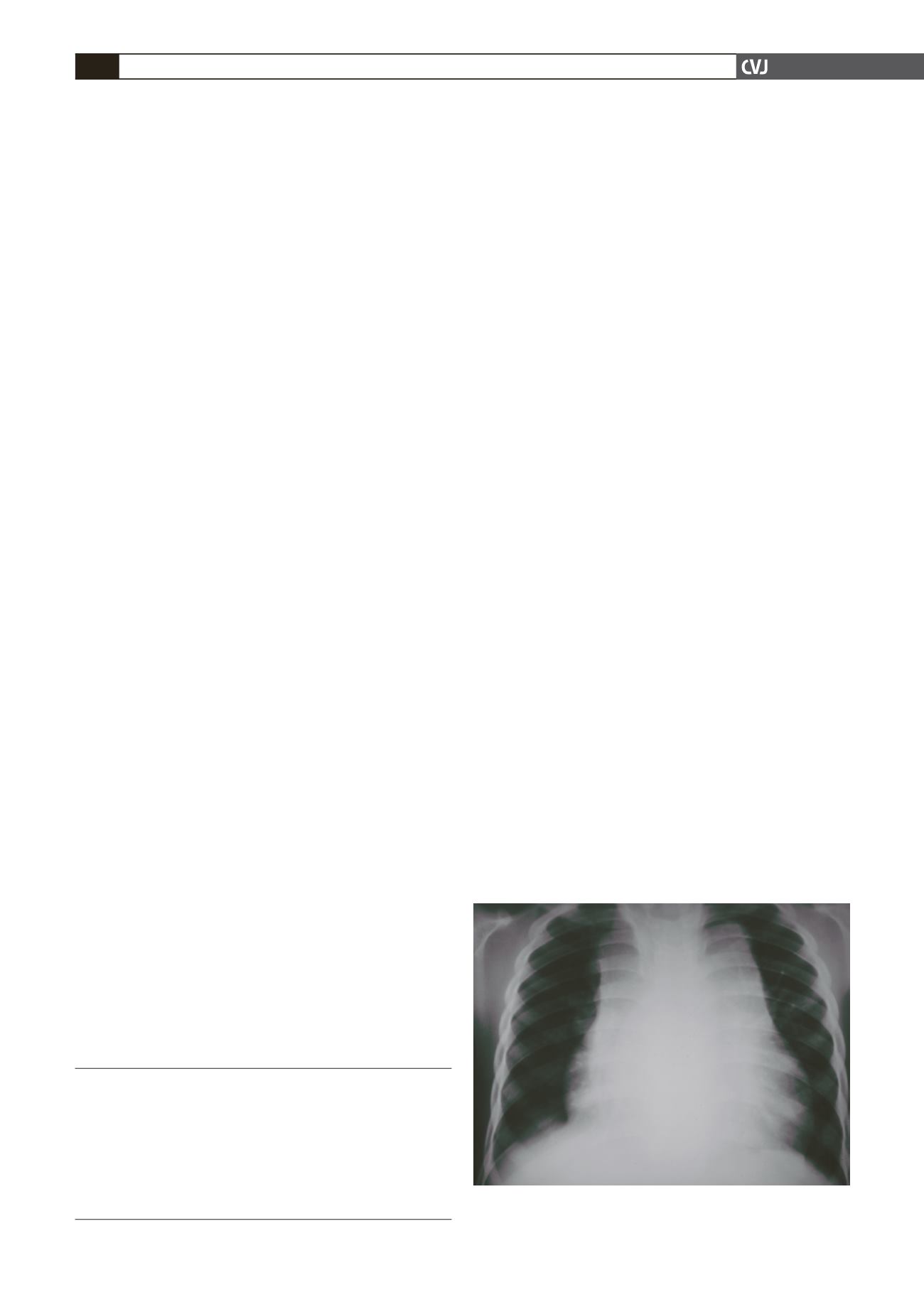
conduction anomalies or repolarisation changes. The postero–
anterior chest X-ray showed marked enlargement of the supe-
rior mediastin and cardiomegaly (Fig. 1). Laboratory work up
revealed a white blood cell count of 14 600 cells/
μ
l, haemoglobin
10.3 g/dl with mean corpuscular volume 60 fl and mean concen-
tration of haemoglobin 20.7 g/dl, platelet count 491 000 /
μ
l,
erythrocyte sedimentation rate (ESR) 16 mm, C-reactive protein
(CRP) 97.4 mg/l, normal renal and liver function, spontaneous
INR of 1.5 and mild hypoalbuminaemia. The HIV serology and
tuberculin reaction were negative.
Transthoracic echocardiographic examination revealed a
40-mm diameter mobile homogeneous mass in the right atrium
attached to the interatrial septum, partially obstructing the
tricuspid valve, and hindering the filling of the right ventricle
(Fig. 2a). There was infiltration of the ventricular myocardium
in the interventricular septum, the interatrial septum, the area
surrounding the aortic valve and the right ventricular outflow
tract, without any significant obstruction (Fig. 2b). There was
also a moderate fibrinous pericardial effusion. Additionally,
several masses were visible in the mediastin, causing distortion
of the contour of the great vessels.
An abdominal echocardiography confirmed the presence of
congestive hepatomegaly, slightly enlarged spleen with numer-
ous micronodules measuring less than a centimetre, and mild
Instituto do Coração, Maputo, Mozambique
AO MOCUMBI, MD, PhD
L PAUL, MD
MB FERREIRA, MD, PhD
Hospital Geral de Mavalane, Mozambique
L MACIEL, MD
Hospital Central de Maputo, Mozambique
P SILVA, MD
Fig. 1. Chest X-ray showing mediastinal enlargement and
cardiomegaly.


