CARDIOVASCULAR JOURNAL OF AFRICA • Vol 22, No 4, July/August 2011
194
AFRICA
Several surveys and studies into the prevalence of risk factors
of atherosclerotic disease in Sudan were conducted in recent
years. The SHHS showed a self-reported prevalence of hyper-
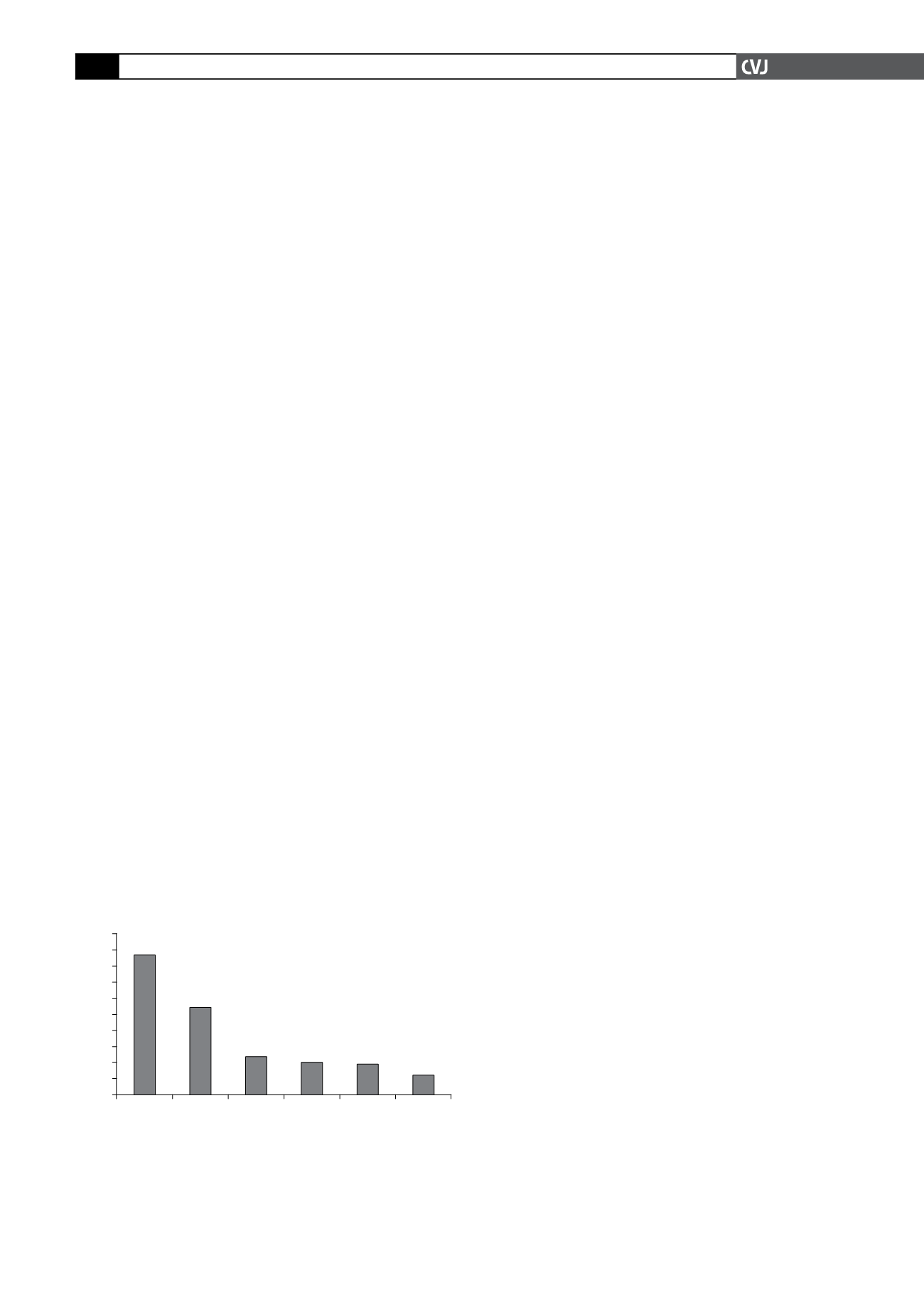
tension and DM of 20.4 and 12.7%, respectively. The STEPS
survey
41
of chronic risk factors for IHD, carried out in Khartoum
state from December 2005 to January 2006 showed high preva-
lence rates of these risk factors. Fig. 3 illustrates prevalence rates
for hypertension, DM, obesity, hypercholesterolaemia, smoking
and physical inactivity in the STEPS survey.
The high prevalence of these risk factors is alarming. The
INTERHEART study showed that the nine risk factors (smoking,
diabetes, hypertension, increased ratio of apolipoprotein B to
apoliporotein A-1, increased weight-to-hip ratio, low consump-
tion of fruits and vegetables, low physical activity, no alcohol
intake and psychosocial stress) provided population-attributable
risk (PAR) for developing a first-time myocardial infarction of
90.4% worldwide
42
and 97.4% in Africa.
24
Of these risk factors,
only five (current/former tobacco smoking, self-reported diabe-
tes and hypertension, abdominal obesity measured as waist-to-
hip ratio, and elevated ApoB/ApoA-1 ratio) accounted for 78.4%
of the PAR worldwide
42
and 89.2% in the African participants.
24
Cardiomyopathies
Idiopathic dilated cardiomyopathy (DCM)
Idiopathic DCM is a major cause of heart failure in Africa.
43,44
However, there are no population-based data on the burden of
the disease in Africa and most data come from hospital-based
surveys.
Earlier hospital-based surveys show that cardiomyopathies
constitute 4 to 6% of all cardiac admissions.
16
In our cardiology
unit at the Al Shaab Teaching Hospital in Khartoum, where the
National Cardiothoracic Centre is located, 12% of all admis-
sions in 2009 were due to idiopathic DCM. Many clinicians in
Sudan believe that DCM is becoming more prevalent. Lack of
epidemiological data that support such assumptions hinder the
recognition of this disease as a major health issue.
Endomyocardial fibrosis (EMF)
No epidemiological data are available on the prevalence of
EMF in Sudan. Limited data are available from hospital-based
surveys. In adults it seems to be a rare cause of heart disease.
15
In the paediatric population, it appears to be a more important
cause. Ali reviewed all paediatric patients with cardiac disease
admitted at the Children’s Hospital, Khartoum from September
2007 to September 2008 and identified six patients with EMF,
constituting 18% of all children with cardiomyopathy.
45
Peripartum cardiomyopathy (PPCM)
The only data on the incidence of PPCM come from unpublished
work by Kineish
et al.
All deliveries in Khartoum Teaching
Hospital from 1975 to 1979 were screened. Any woman who
developed heart failure during the last trimester or during puer-
perium was examined clinically, and evaluated by electrocardio-
gram and chest X-ray. If no identifiable cause of heart failure
was found, patients were labelled as having PPCM. Thirteen
patients were identified out of 8 605 deliveries, with an incidence
of 1.5 in 1 000 deliveries. This is similar to the incidence in the
sub-Saharan region, except possibly in the Zaria province in
northern Nigeria, which has the highest reported incidence rate
of one in 100 deliveries.
46,47
Congenital heart disease
The prevalence of congenital heart disease among schoolchildren
aged five to 15 years was studied as part of phase 1 of the WHO
Global Rheumatic Fever/Rheumatic Heart Disease Prevention
Programme in Sudan. There were 27 cases of congenital heart
disease found in a total of 13 322 children screened, giving a
prevalence rate of 2.0 per 1 000 children. The rate is comparable
to that of similar African countries but lower than European and
North American rates.
49-53
Among children admitted to hospital, congenital heart disease
is the commonest cause of heart disease, followed by rheumatic
heart disease and cardiomyopathy. Ventricular septal defect,
atrial septal defect, tetralogy of Fallot, patent ductus arteriosus
and pulmonary stenosis were the commonest diseases.
54,55
Conclusion
Heart disease is prevalent in Sudan, with at least 2.5% of the
population affected, and it is one of the major causes of hospital
mortality. The tetrad of hypertensive heart disease, ischaemic
heart disease, rheumatic heart disease and cardiomyopathy
constitute the bulk of heart disease.
Hypertension is prevalent, especially in urban communities,
with poor control rates. Data on RHD are only available for
the capital state of Khartoum, where a prevention programme
succeeded in reducing prevalence 10-fold from 3/1 000 to 0.3/
1 000 population. There are no recent epidemiological data on
the prevalence of IHD. However, IHD risk factors are alarmingly
prevalent in the community.
Prevalence of cardiomyopathies is not known, although it
seems clinicians are recognising idiopathic dilated cardiomyo-
pathy more frequently. EMF is rarely reported in adult patients
in recent literature but is seen infrequently in paediatric popula-
tion. Peripartum cardiomyopathy seems to occur at a similar
incidence to that in other sub-Saharan countries. The prevalence
rate of congenital heart disease is comparable to other African
countries but lower than European and North American rates.
Epidemiological data are scarce and fragmented.
The need for quality data cannot be overemphasised. However,
Fig. 3. Results of STEPS survey in Sudan 2005/2006.
100
90
80
70
60
50
40
30
20
10
0
% of total population
86.8
53.9
23.6
19.8
19.2
12
Source: World Health Organisation. Available at http://
Low
physical
activity
Over-
weight &
obesity
Hyper-
tension
Hyper-
chole-
sterol-
aemia
Diabetes Smoking


