CARDIOVASCULAR JOURNAL OF AFRICA • Vol 22, No 6, November/December 2011
AFRICA
e1
Case Report
A giant pericardial cyst
İSLAM KAKLIKKAYA
Abstract
Pericardial cysts are rare, benign, congenital anomalies. Most
are asymptomatic and are found incidentally on chest radio-
graphs. Some may cause symptoms and complications. Giant
pericardial cysts are even more rare, and few reports on their
natural history, presentation and management are available.
This report describes a giant pericardial cyst that exerted
pressure on the heart and lungs and was excised surgically.
Subsequently, the patient has been asymptomatic for nine
years and appears to be in complete remission.
Keywords:
pericardial cyst, surgical treatment
Submitted 7/1/10, accepted 31/8/10
Cardiovasc J Afr
2011;
22 (6)
: online publication
DOI: 10.5830/CVJA-2010-076
Pericardial cysts are caused by the incomplete coalescence of
foetal lacunae during the development of the pericardium.
1
They
are usually unilocular, well-marginated, spherical or teardrop-
shaped cysts that may be attached to the pericardium directly
or by a pedicle.
2
Pericardial cysts are lined by endothelium or
mesothelium and contain clear serous fluid (‘spring water’).
These cysts do not connect with the pericardial space.
They are asymptomatic in more than 50% of cases and are
detected incidentally on chest X-ray. They are generally more
likely to be found in middle-aged adults, most frequently in the
third or fourth decade of life, and equally in men and women.
3
Some pericardial cysts may cause symptoms and complications
such as right ventricle outflow obstruction, pulmonary stenosis,
pericardial tamponade and partial erosion of the superior vena
cava.
4
Case report
The patient was a 39-year-old man who had reported several
episodes of left pleuritic chest pain and who had been diagnosed
elsewhere with a Morgagni diaphragmatic hernia. His medical
history included severe hypertension (220/120 mmHg). The
patient was generally active and was otherwise in good health.
He had smoked one packet of cigarettes daily for 25 years, and
had a dry cough. He had had palpitations, non-specific gastroin-
testinal system complaints, nausea, vomiting and dyspepsia for
five years. He had seen many doctors, including psychiatrists,
for these complaints. He was transferred from a state hospital to
our clinic with the working diagnosis of diaphragmatic hernia for
surgical treatment.
On examination, he was in no distress. His blood pressure
was 180/90 mmHg, the heart rate was 90 beats/min, and he had a
regular heartbeat with normal heart sounds and no murmurs. An
electrocardiogram revealed a sinus tachycardia and non-specific
ST-T changes in V5–6.
The breath sounds were absent on auscultation of the lower
two-thirds of the left hemithorax. On percussion, there was dull-
ness in the fifth left intercostal area, which indicated Traube’s
space was obliterated.
He was afebrile, acyanotic, normal coloured and anicteric. No
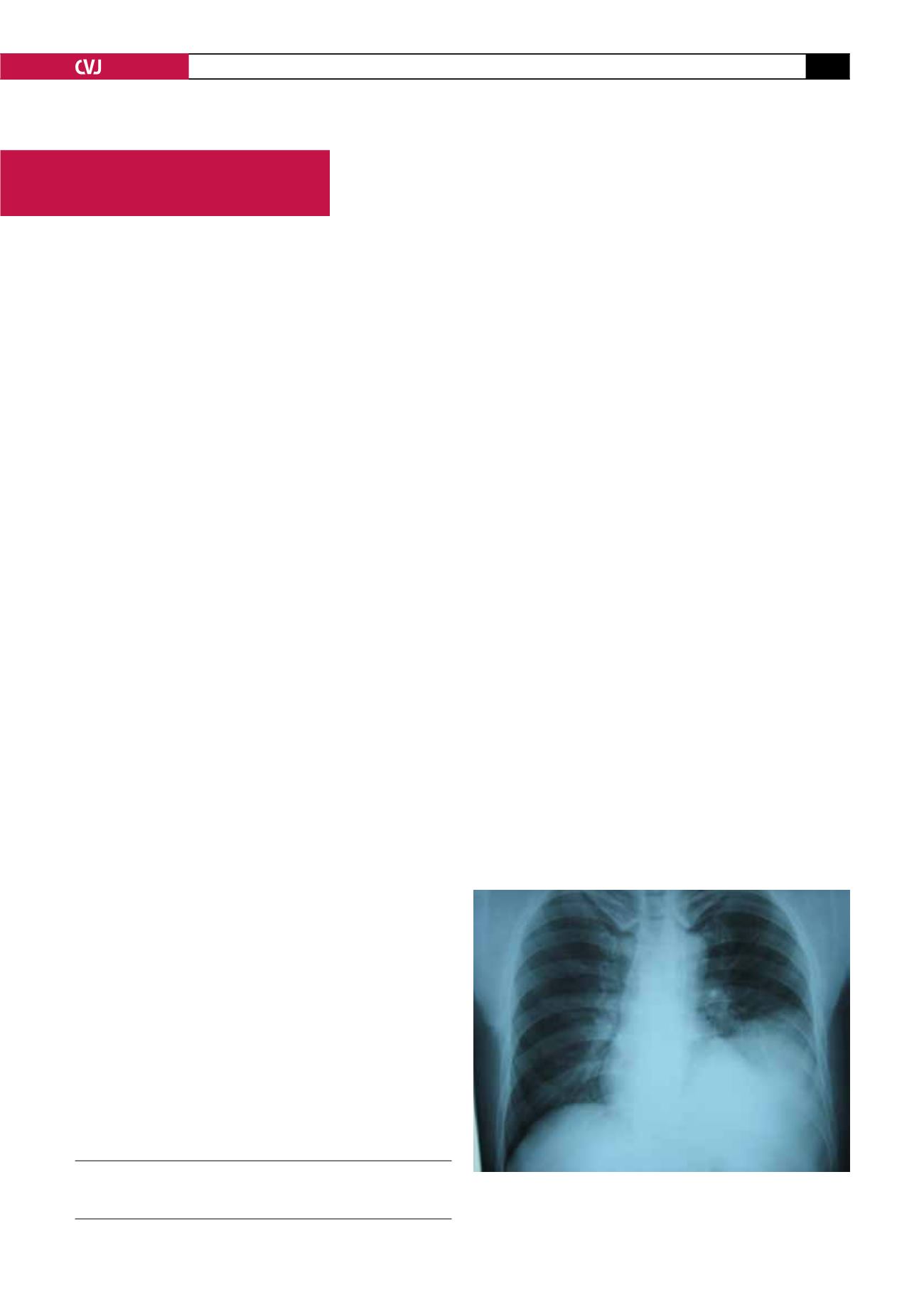
jugular venous distention was seen. The postero-anterior chest
X-ray showed atelectasis of the inferior lobe of the left lung,
caused by a mass in the left hemithorax, massive pleural effusion
in the left lower hemithorax, and mild cardiomegaly (Fig. 1).
Routine laboratory tests were unremarkable. The purified
protein derivative of tuberculin test was equivocal.
The transthoracic echocardiogram suggested that the mass
was a thin-walled, cyst-like structure adherent to the left ventri-
cle. No intracardiac masses or other echocardigraphic abnormal-
ities such as a prominent fad pad, solid tumour, aortic aneurysm,
left ventricle aneurysm and prominent left atrial appendage were
found.
Subsequent contrast-enhanced computed tomography (CT)
revealed a cystic mass in the left mediastinum above the
diaphragm, surrounding the left cardiac border (Fig. 2). The
mass measured 22
×
15
×
17 cm (transverse
×
anteroposterior
Department of Cardiovascular Surgery, School of Medicine,
Karadeniz Technical University, Trabzon, Turkey
İSLAM KAKLIKKAYA, MD, PhD,
Fig. 1. The postero-anterior chest radiograph shows a
large, homogeneous radiodense mass in the basal left
hemithorax.


