


















 35 / 64
35 / 64

AFRICA
S33
CVJAFRICA • Volume 26, No 2, H3Africa Supplement, March/April 2015
In the Tanzanian community-based incident stroke study
(2003), case fatality rate was 28.7% at 28 days and 84.3% at three
years. The 28-day case fatality rate was at the lower end of rates
reported for other LMIC, even when including those identified
by verbal autopsy, while the three-year case fatality rates were
notably higher than seen in most developed-world studies.
Recent studies from the developed world suggest three-year case
fatality rates of 43 to 54% and five-year case fatality rates of 53
to 60%.
32
In a South African study (published in 2012), 25.5% of
patients died within three months of discharge and 38% within
the 12-month follow-up period.
58
This high fatality rate may be
due to the severe scarcity and prohibitive costs of facilities and
human resources for investigations, acute care and rehabilitation
of stroke patients in Africa.
6
The region has the lowest
neurologist-to-population and doctor-to-population ratio in the
world,
6
with an average of one neurologist to one million people
in comparison to one to 100 000 in high-income countries.
6
With high proportion of the population living below the
poverty line, the few available facilities for investigation and care
of stroke patients are not accessible to most of the population
who have to pay out of their pockets.
6,59
For instance, there is
probably only one multidisciplinary holistic neuro-rehabilitation
centre in East, West and Central Africa.
60, 61
Disability-adjusted life years
Direct studies of DALYs due to stroke are very rare in Africa.
The burden of disease due to stroke in South Africa (2008) was
564 000 DALYs.
62
Of this, 17% was contributed by years lost to
disability (YLD) (14–20% in sensitivity analysis).
62
The estimated
DALYs lost due to stroke was 1 230 per 100 000 in Angola,
Africa, compared to 200 per 100 000 in Switzerland, Europe in
2002.
53,63
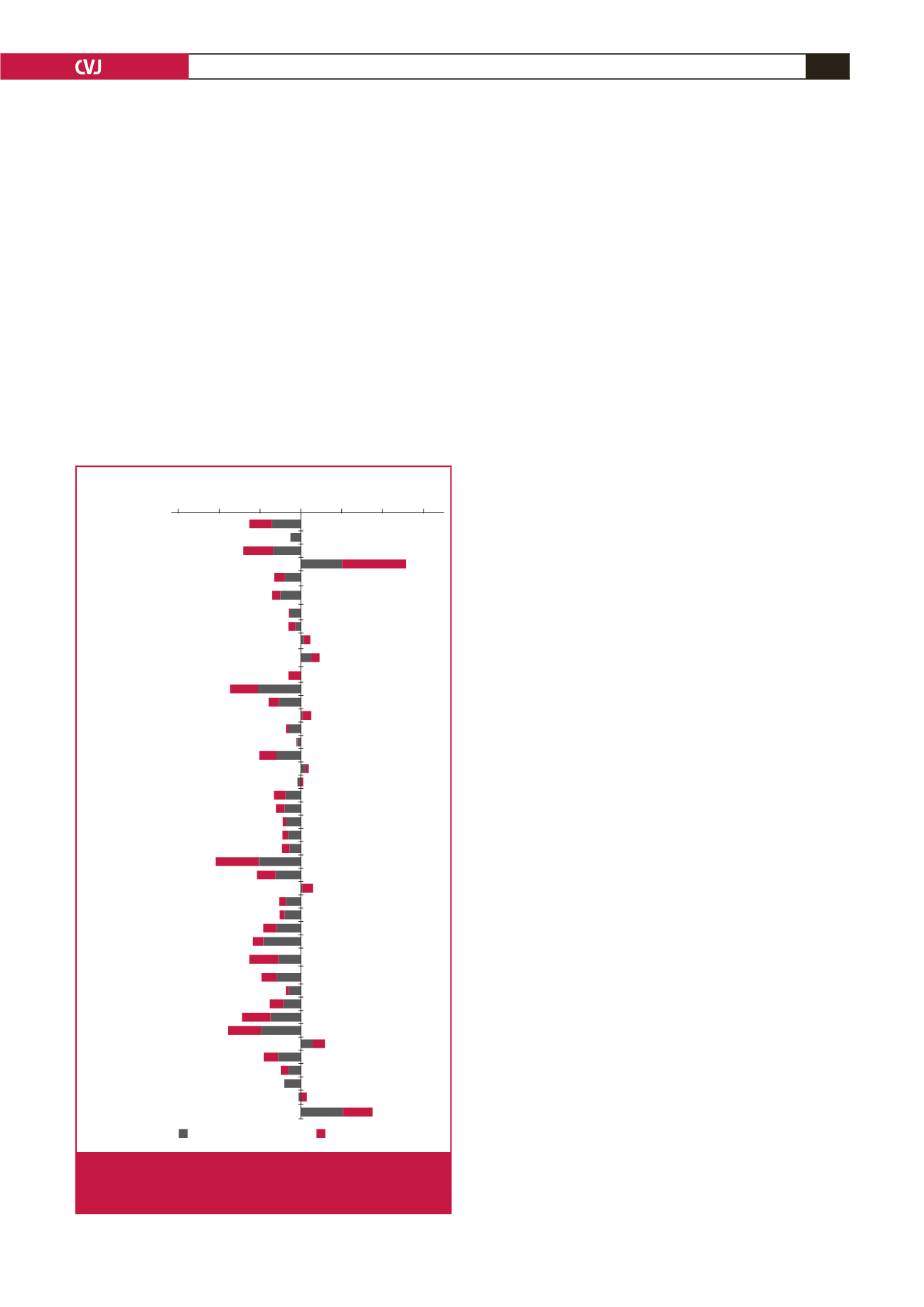
Using the GBD data (Table 3, Fig. 4), percentage change in
age-standardised ischaemic stroke DALYs from 1990 to 2010
ranged between –53.1 (Mauritius) and 79.0 (Burkina Faso).
Overall, in Africa, there was significant (
p
<
0.001) median
change in age-standardised ischaemic stroke DALYs of –10.31
between 1990 and 2010. Similarly (Table 3, Fig. 7), change
in age-standardised haemorrhagic stroke DALY for the same
period ranged between –53.8 (Equatorial Guinea) and 51.6
(Zimbabwe).
Overall, in Africa, there was a statistically significant (
p
<
0.001) median change in age-standardised haemorrhagic
stroke DALYs of –18.9 between 1990 and 2010. However,
stroke remained the leading cause of cardiovascular DALYs in
sub-Saharan Africa, increasing from 5 930 040 (39.5%) in 1990
to 7 824 920 (52.0%) of CVD DALYs in 2010.
3
Stroke type and risk factors
The proportion of haemorrhagic stroke in Africa ranges from 29
to 57%, in comparison with 16 to 20% in North America.
53
In the
INTERSTROKE study, haemorrhagic stroke was 34% in Africa
and 9% in high-income countries.
56
This suggests a higher burden
of uncontrolled hypertension in Africa, because the proportion
of haemorrhagic stroke in a population seems to correlate with
the prevalence and severity of uncontrolled hypertension.
16,32,53-55
Up to 98% of stroke patients in Africa have hypertension.
32,53,55
Ischaemic stroke is more associated with diabetes mellitus,
cardiac disease, age above 61 years and previous transient
ischaemic attacks.
54
The population-attributable ratio of stroke
due to hypertension in South Africa in 2000 was 50%,
64
and 60%
in North Africa.
65
Hypertension
Hypertension, once rare in West Africa, is emerging as a serious
endemic threat. It has been referred to as a silent killer, as it often
has no early detectable symptoms despite being a major cause
of serious health conditions, including heart disease, stroke and
renal disease.
66
Of the 10 predominant modifiable risk factors
accounting for 90% of the risk of stroke, hypertension is the
strongest.
56
Prevalence rates for hypertension vary across and within
regions in Africa. An analysis of all national data in Zimbabwe
in the 1990s found that between 1990 and 1997, the national
Algeria
Benin
Botswana
Burkina Faso
Burundi
Central African
Republic
Chad
Congo
Côte d’Ivoire
Democratic
Republic of Congo
Egypt
Equatorial Guinea
Ethiopia
Ghana
Guinea
Guinea-Bissau
Kenya
Lesotho
Liberia
Libya
Madagascar
Malawi
Mali
Mauritania
Mauritius
Morocco
Mozambique
Namibia
Niger
Nigeria
Rwanda
São Tomé
and Príncipe
Senegal
Sierra Leone
Somalia
South Africa
Sudan
Swaziland
The Gambia
Togo
Uganda
Zambia
Zimbabwe
–150 –100 –50 0
50 100 150
Country
Haemorrhagic stroke
Ischaemic stroke
% Change in DALYS
Fig. 4.
Model-derived percentage changes in ischaemic
and haemorrhagic stroke disability-adjusted life years
(DALYs) in African countries between 1990 and 2020.