
















 11 / 76
11 / 76

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 28, No 1, January/February 2017
AFRICA
9
Methods
This was a prospective cohort study conducted at Parirenyatwa
Hospital, a tertiary-care teaching hospital in Harare, Zimbabwe.
The study protocol was approved by the Joint Parirenyatwa
Hospital and College of Health Sciences Research ethics
committee as well as the Medical Research Council of Zimbabwe.
Informed consent was given by all patients.
Consecutive patients seen between 1 August 2012 and 31 July
2013 in the echocardiography clinic at Parirenyatwa Hospital
who fulfilled the entry criteria were enrolled into a detailed
PPCM registry. Inclusion criteria were: women aged 16 to 49
years; development of symptoms of heart failure one month
prior to and up to five months after delivery where no obvious
cause could be established; left ventricular systolic dysfunction
with ejection fraction (EF)
<
45% or fractional shortening (FS)
<
30% on transthoracic echocardiograph. Exclusion criteria were:
significant organic valvular disease; systolic blood pressure
>
160
mmHg and/or diastolic blood pressure
>
100 mmHg.
On enrolment, the following was obtained for each case:
demographic data, medical and obstetric histories, drug therapy,
clinical examination findings and echocardiographic profile.
After the initial assessment, these patients were subsequently
followed up and managed for six months at the cardiac clinic at
Parirenyatwa Hospital.
The two time points that were of interest for this study were three
and six months after enrollment. At each time point the NYHA
functional class and drug management were assessed. In addition,
a thorough clinical examination was carried out and clinical data
were recorded. Echocardiography to assess left ventricular function
was repeated at the three- and six-month reviews.
Two-dimensional and targeted M-mode echocardiography
was performed using a Hitachi EVB 7500 ultrasound scanner.
Echocardiograms were carried out with patients in the left lateral
decubitus position. Left ventricular ejection fraction (LVEF)
was calculated using left ventricular internal systolic (LVDs) and
diastolic dimensions (LVDd). These were measured at the level
of the mitral valve leaflet tips in the parasternal long-axis view
in accordance with the American Society of Echocardiography
guidelines.
15
A rhythm ECG strip was recorded during
echocardiography and LVDd was determined in M-mode at the
beginning of the Q wave, and LVSd was determined at the end
of the T wave. The valves were carefully interrogated in the four
standard views to determine morphology.
Echocardiography was performed by cardiologists or senior
clinicians at enrolment and at the six-month review. The three-
month studies were performed by the investigator using a mobile
Sonosite ultrasound machine and images were recorded and
subsequently reviewed by a cardiologist or senior clinician for
accuracy of measurements.
Remarkable recovery was defined as an increase in the
LVEF
>
20% from baseline and complete recovery as LVEF
>
50% after six months. The investigator assigned the NYHA
functional class for each patient at baseline and at subsequent
follow-up visits. Patients were defined as improvers if they were
in functional class I or II or had improved by at least one class at
the end of the six-month period.
Statistical analysis
Study data were collected andmanaged using Research Electronic
Data Capture (REDCap), a secure web-based application
designed to support data capture for research studies,
16
hosted at
the University of Zimbabwe College of Health Sciences. These
data were exported and analysed using the STATA statistical
package (version 10.1, College Station, TX). Discrete variables
are presented as
n
(%), and continuous variables are presented
as mean
±
standard deviation. A paired ANOVA test was used
to compare ejection fraction at baseline and after three and
six months. Fisher’s exact test was used to compare NYHA
functional class at baseline and after three and six months.
Significance was defined as a two-tailed
p
-value
<
0.05 unless
otherwise specified.
Results
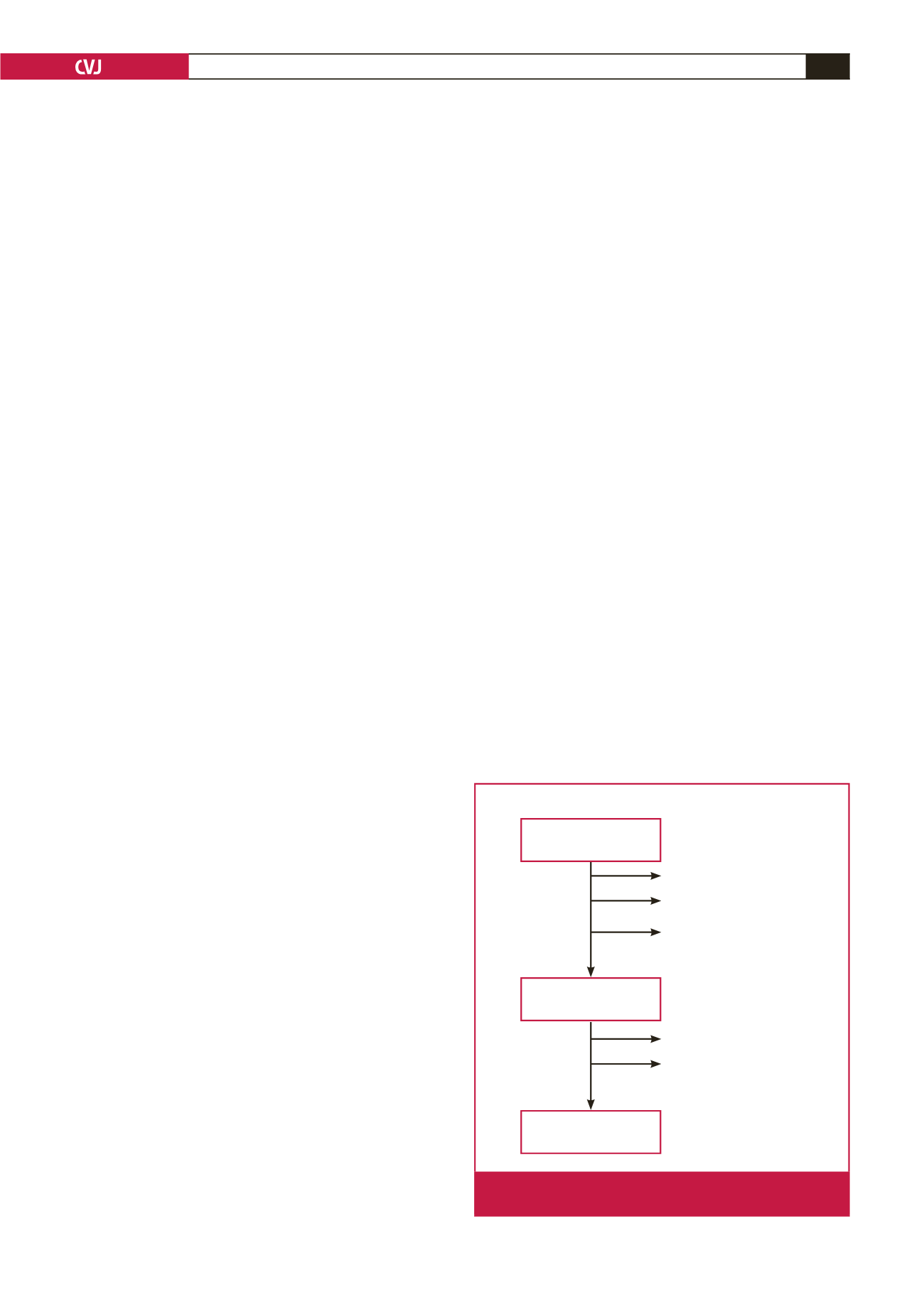
A total of 43 patients were enrolled into the study (Fig. 1). Only
one patient was lost to follow up. Left ventricular function at
three months could not be assessed for one patient because she
did not come for the review, although she had an echocardiogram
performed at six months. Two patients missed the six-month
review so clinical assessment and echocardiography could not
be done. However both patients were contactable by phone and
were reported to be alive and well.
Table 1 shows the baseline demographic and clinical
characteristics of the patients. The mean age of the cohort
was 27.9
±
6.0 years. The majority of patients (15, 34.9%) were
primigravida, with seven (16.3%) having a parity of four or more.
At enrolment, 23 (53.5%) of the patients were NYHA class II,
with only seven (16.3%) having an NYHA class of IV.
A relatively large proportion (15, 34.9%) of the cohort
had been diagnosed with and managed for pregnancy-induced
hypertension. Out of all 43 patients, three had twin deliveries.
Only one (2.3%) patient admitted to having symptoms of heart
failure two weeks prior to delivery compared to 40 (93.0%)
At baseline
At 3 months
At 6 months
43 patients enrolled
37 patients returned
for follow up
35 patients returned
for follow up
4 deaths
1 death
1 lost to follow up
1 missed 3-month follow up
but contactable by phone
2 missed 6-month follow up
but contactable by phone
Fig. 1.
Study flow diagram of 43 participants with newly diag-
nosed PPCM.