
















 33 / 74
33 / 74

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 30, No 2, March/April 2019
AFRICA
99
were found to have significantly increased TG, TC, low-density
lipoprotein cholesterol (LDL-C) and high-density lipoprotein
cholesterol (HDL-C) levels when compared to the ART-naïve
patients.
41
However in another study, patients on ART for less
than two years had relatively less risk of dyslipidaemia than
those on it for longer.
42
In the present study, ART demonstrated
no significant effect on lipid profiles. This lack of effect may be
due to the fact that changes in lipid profiles have been noted
mostly in ART treatment other than the FDC used in this study,
43
or the relatively short treatment period.
44
Rooibos consumption exerted TC-lowering effects in this
study; however, the other blood lipid parameters were unaffected.
Lipid lowering with rooibos intake has been seen in both humans
and rats.
45,46
No significant differences were found in the TBARS levels
between the groups. This was partially unexpected as ART
(particularly PI and EFV) has previously been found to increase
TBARS in both cell-based and epidemiological studies.
45,47-49
On the other hand, our findings do not contradict those of an
epidemiological study by Masia
et al.
,
46
who showed increased
oxidative stress by lipid peroxidation in subjects receiving
PI-containing ART, while ART containing NNRTIs (including
EFV), such as in our study, induced oxidative stress levels similar
to those observed in ART-naïve patients.
46
A study in rat testes
showed no increase in TBARS in testicular tissue after eight weeks
of therapy with the same FDC as was used in the present study.
50
The noveltyof our findings provides insight on the effects of the
EFV/FTC/TDF combination drug. From the results, it appears
that this specific FDC is possibly not associated with increased
lipid perdoxidation, as seen in other previously investigated
combinations, or that it would need a longer treatment period to
exert observable changes in lipid peroxidation.
Improved antioxidant capacity due to rooibos and the ability
of rooibos to inhibit lipid peroxidation has been demonstrated in
several studies.
28,51-54
However, it has also been shown to have no
effect in other studies.
34,55
Conducting one or two complementary
techniques, such as determination of the total antioxidant
capacity together with the TBARS analysis may have provided
a more cohesive insight on the antioxidant capacity of the rats.
However, our results seem to be similar to those of other studies
in that rooibos treatment did not adversely affect oxidative stress.
Coronary flow in ART-exposed animals was lower than in
the ART animals supplemented with rooibos. A decrease in
myocardial perfusion was observed during ART in a longitudinal
study in humans with positron emission tomography and flow-
mediated dilation, where myocardial perfusion was seen to
decrease.
56
Although a significant decrease in coronary flow from
control values in either the ART or the ART + rooibos groups
was not seen in this study, the ability of rooibos co-treatment
with ART to significantly improve coronary flow compared to
ART only is, as far as we are aware, a novel finding.
Certain flavonoids, such as quercetin, which are found
in rooibos, have been shown to increase endothelial nitric
oxide synthase 3 (eNOS) activity and endothelium-dependent
vasorelaxation in aortic rings from spontaneously hypertensive
rats.
57
However, this is the first time rooibos has been directly
linked to increased coronary flow in the baseline (pre-ischaemic)
setting, specifically in the context of ART, and further
investigations are warranted to explore underlying mechanisms.
Interestingly, no other functional parameters (pre- and post-
ischaemia) or percentage recovery values were affected by either
rooibos or ART, or in combination. Although difficult to
explain, it may be due to a too-short treatment period that was
not sufficient to elicit functional effects in the hearts, despite
showing demonstrable effects in terms of infarct size and vascular
function, as discussed below. It is also possible that the FDC takes
longer to provoke functional changes in the heart. Furthermore,
the majority of previous studies investigated the effects of PIs
in
vivo
or
in vitro
, or the effect of NRTIs and NNRTIs in the
ex vivo
setting or on organs other than the heart.
16,57,58
The infarct size of the ART treated group was significantly
greater than that of the control group, which suggests that, in
our hands, the TDF/FTC/EFV combination treatment was
associated with decreased myocardial ischaemic tolerance. This
may be explained by an ART-induced reduction in cell viability
as a result of toxicity. EFV, particularly, has previously been
demonstrated to result in endoplasmic reticulum stress-induced
apoptosis and therefore decreased cell viability in human brain
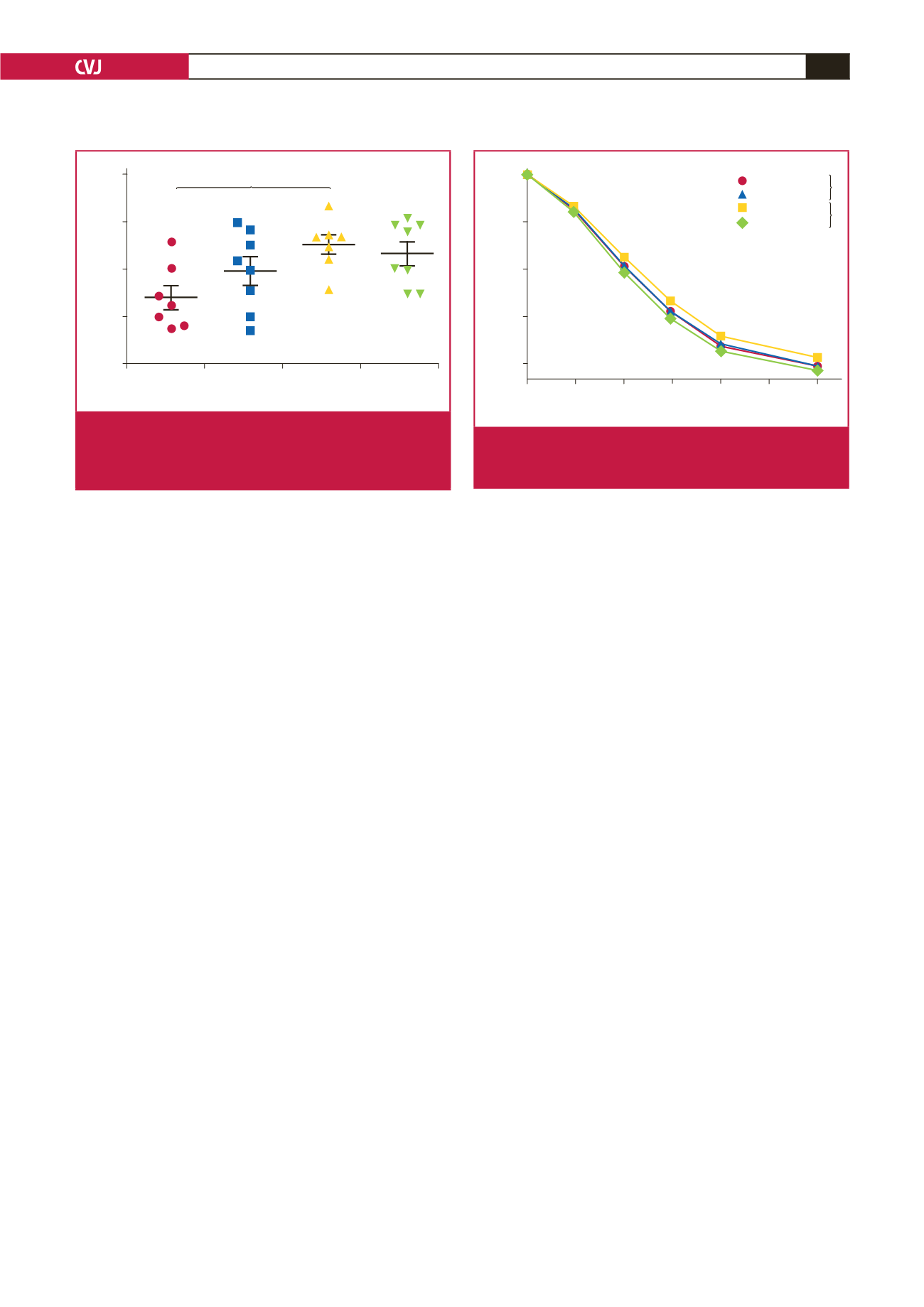
Treatment group
Control
Rooibos
ART ART + rooibos
Infarct size (% AAR)
80
60
40
20
0
*
Fig. 3.
Infarct size expressed as a percentage of the area at
risk (%AAR) at the end of the nine-week treatment
period. One-way ANOVA with Bonferonni
post hoc
test, *
p
<
0.05;
n
=
seven to eight per group.
Acetylcholine (M)
1.0
×
10
–8
3.2
×
10
–8
1.0
×
10
–7
3.2
×
10
–7
1.0
×
10
–6
3.2
×
10
–6
1.0
×
10
–5
% Relaxation
0
25
50
75
100
Control
Rooibos
ART
Rooibos + ART
*
**
Fig. 4.
Ach-induced relaxation of aortic rings at the end of the
nine-week treatment period;
n
=
20 to 25 per group; *
p
<
0.05; two-way ANOVA, **
p
<
0.01.