
















 5 / 68
5 / 68

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 30, No 3, May/June 2019
AFRICA
133
Cardiac rehabilitation delivery in Africa
Martin Heine, Karam Turk-Adawi, Marta Supervia, Wayne Derman, Francisco Lopez-Jimenez, Pamela
Naidoo, Sherry L Grace
As of 2011, the leading cause of premature mortality in
Africa is non-communicable rather than communicable disease
(HIV/AIDS, tuberculosis). The burden of non-communicable
diseases (NCDs), and cardiovascular disease (CVD) specifically,
is growing exponentially in Africa (Fig. 1), at a rate exceeding
that globally.
1,2
Mortality rates for NCDs in sub-Saharan Africa
already exceed those for the global population across most age
groups (Fig. 2). Given that CVD onset and mortality are often
premature, this exponential rise will limit poverty-reduction
initiatives and economic development.
3-5
Keywords:
cardiac rehabilitation, myocardial ischaemia, non-
communicable diseases, Africa
Submitted 13/12/18, accepted 26/2/19
Published online 27/3/19
Cardiovasc J Afr
2019;
30
: 133–137
www.cvja.co.zaDOI: 10.5830/CVJA-2019-011
Cardiac rehabilitation (CR) is an established model of care
designed to mitigate the burden of NCDs, and CVD specifically.
6,7
CR is a multi-component programme, delivering structured
exercise, education and risk-factor management, largely by
non-physician health workers, such as a community healthcare
worker, allied healthcare provider or nurse.
8,9
Robust evidence
from predominantly high-income countries demonstrates that CR
is associated with a reduction in rates of cardiovascular mortality
(by 26%) and re-hospitalisation (by 18%), as well as increases
in quality of life, while being cost effective.
6,7
Available evidence
from low- and middle-income countries (LMICs) corroborates
these benefits.
10
CR is a recommendation in clinical guidelines for,
among others, ischaemic heart disease (IHD) patients.
8,11-13
Global study on CR availability and character-
istics
Under the auspices of the International Council for Cardiac
Prevention and Rehabilitation (ICCPR), Grace
et al
. recently
(2017) set out to rigorously establish the availability, capacity
Institute of Sport and Exercise Medicine, Faculty of Health and
Medicine, Stellenbosch University, Cape Town, South Africa
Martin Heine, PhD,
mheine@sun.ac.zaWayne Derman, MD, PhD
Department of Physiotherapy, Faculty of Health and
Medicine, Stellenbosch University, Cape Town, South Africa
Martin Heine, PhD,
mheine@sun.ac.zaQatar University, Doha, Qatar
Karam Turk-Adawi, PhD
Gregorio Marañón Health Research Institute, Gregorio
Marañón General University Hospital, Madrid, Spain
Marta Supervia, MD
Division of Preventive Cardiology, Department of
Cardiovascular Medicine, Mayo Clinic, Rochester, USA
Marta Supervia, MD
Francisco Lopez-Jimenez, MD, PhD
IOC Research Centre, South Africa
Wayne Derman, MD, PhD
York University; University Health Network, Toronto,
Ontario, Canada
Sherry L Grace, PhD
Heart and Stroke Foundation; African Heart Network;
Department of Psychiatry, Faculty of Health and Medicine,
Stellenbosch University, Cape Town, South Africa
Pamela Naidoo, PhD
Editorial
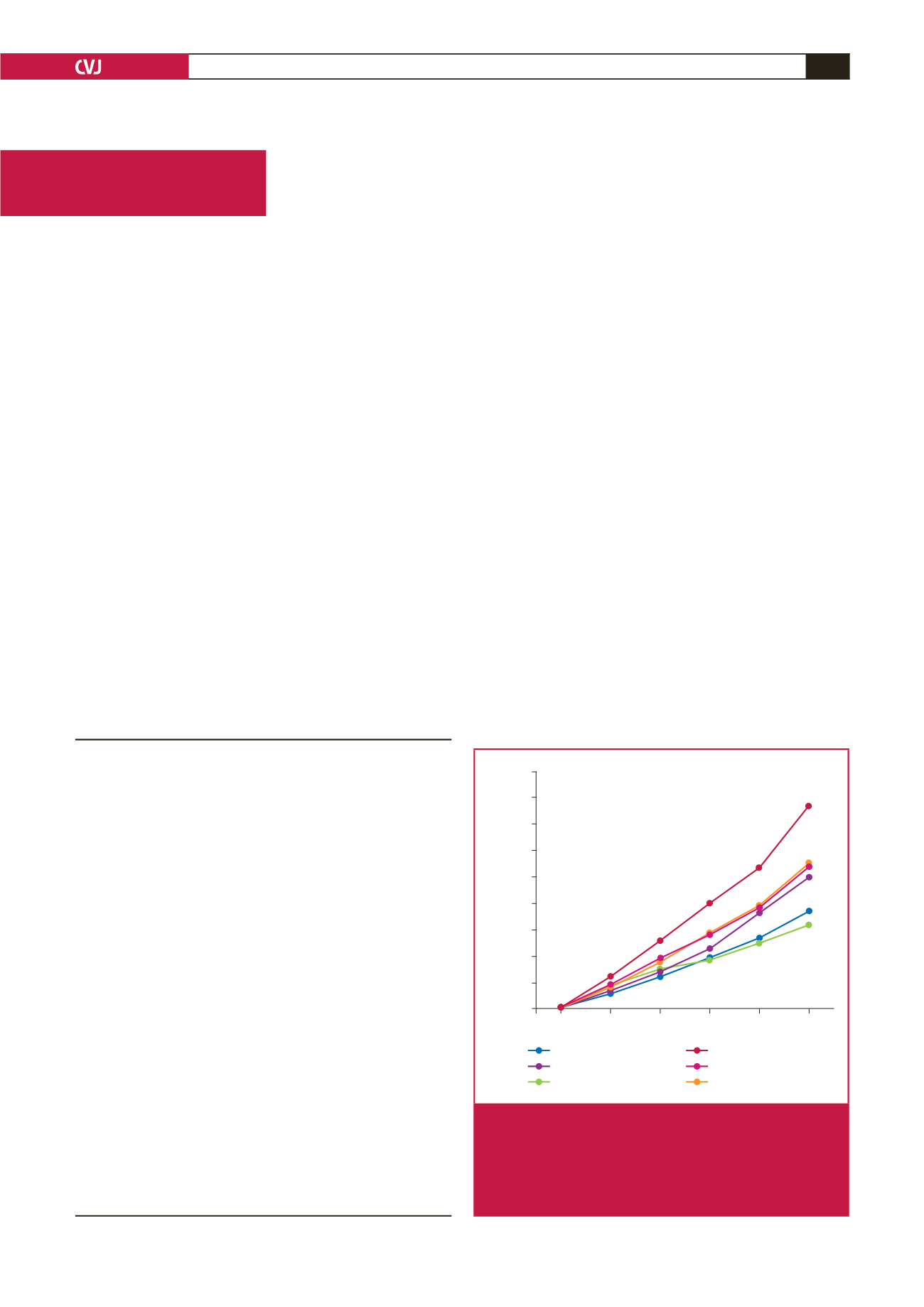
Year
1990 1995 2000 2005 2010 2015
% Change
180
160
140
120
100
80
60
40
20
0
Global
North Africa and Middle East
Central sub-Saharan Africa
Southern sub-Saharan Africa
Western sub-Saharan Africa
Eastern sub-Saharan Africa
Fig. 1.
The global and African change in the incidence of
ischaemic heart disease (IHD) per continental region
from 1990 to 2015, according to the global burden
of disease study.
1
All but the southern sub-Saharan
African region indicated a more rapid increase in the
incidence of IHD relative to global changes.