

















 60 / 70
60 / 70

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 30, No 5, September/October 2019
302
AFRICA
discovery of PCSK9 as a protein that influences LDL receptor
turnover, a therapeutic strategy was developed based on this
action. Although the polygenic nature of FH has been identified
and contributes to the understanding of this clinical phenotype
with high cardiovascular risk, it is possible that more monogenic
causes may be found.
Ideally, a genetic basis should be sought in all patients with
a clinical suspicion of FH, either for a monogenic disorder or
a polygenic form of the disease using a condensed six-SNV
genetic risk score (
CELSR2/SORT1
,
APOB
,
ABCG5/8
,
LDLR
,
and two SNPs in
APOE
). An outline for a diagnostic approach
through genetic testing is presented in Fig. 3. In South Africa,
founder effects may lead to identification of a large number
of patients with a few selected mutations by more traditional
methods, but next-generation sequencing technologies such as
WES offer more extensive screening. In cases where monogenic
FH is excluded, confirmation of polygenic FH would indicate
that cascade genetic testing for identification of affected family
members would not be cost effective. In the remainder of FH
patients without an identifiable mutation, or high polygenic risk
score, additional research for a causal mutation in novel and
unknown gene(s) may be justified.
Much work needs to be done in South Africa for the detection
of monogenic and polygenic FH as a phenotype. The application
of the single-nucleotide variants to the polygenic FH risk score
needs to be confirmed or adapted, to be reliable in populations
with ancestry other than European.
Discussion
The recognition of hypercholesterolaemia and coronary artery
disease in South Africa dates back many years. Prof K Steyn
indicated that Dr Jan Pretorius already drew attention to
dyslipidaemia when it was being recognised by Prof Harry
Seftel with the diagnosis of so many homozygous FH patients
in the region of Johannesburg. Prof Steyn also described work
done at the MRC. In a rural study of Afrikaners and testing
hypercholesterolaemia above the 80th percentile, the prevalence
of FH assessed by the three known mutations in the
LDLR
gene
was one in 72.
The genetic investigation as well as counselling for FH was
discussed. Ms M Schoeman, an experienced HPCSA-registered
genetic counsellor working in Cape Town, indicated that she had
few referrals for counselling and these predominantly related to
inheritance in Afrikaners.
Prof Talmud indicated that founder effects made the detection
of LDL receptor mutations somewhat easier and that next-
generation sequencing could simultaneously provide information
on all FH-associated genes as well as on the genes operating
in polygenic FH. However, in the latter case, the utility of the
polymorphisms used in Europe needs to be established before
applying this set to local dyslipidaemias.
Prof Kotze mentioned that medical schemes controlling
expense for healthcare could consider supporting the analysis
of SNVs, which could identify polygenic FH. This could be
incorporated as part of a pre-screen algorithm for selection of
patients eligible for WES.
The need to develop a local gene score for polygenic FH
was emphasised by Prof Humphries. Prof Raal indicated that
a genetic investigation of six common mutations in the LDL
receptor would be of great help in the diagnosis of FH since there
are strong founder effects in South Africa. Such a diagnostic
service is not available at teaching hospitals. Mutations specific
to regions and ancestral lineage could be selected to make the
genetic diagnosis more cost effective.
The cost of treatment was discussed briefly. The practical
point is that the medical practitioner treats the phenotype
with medication to certain targets, as indicated by the South
African guidelines.
19
The generic statins have made the treatment
much more affordable. Prof Marais indicated atorvastatin and
rosuvastatin should be preferred in the treatment of FH. The
cost of the 80-mg daily dose of atorvastatin is in the range of
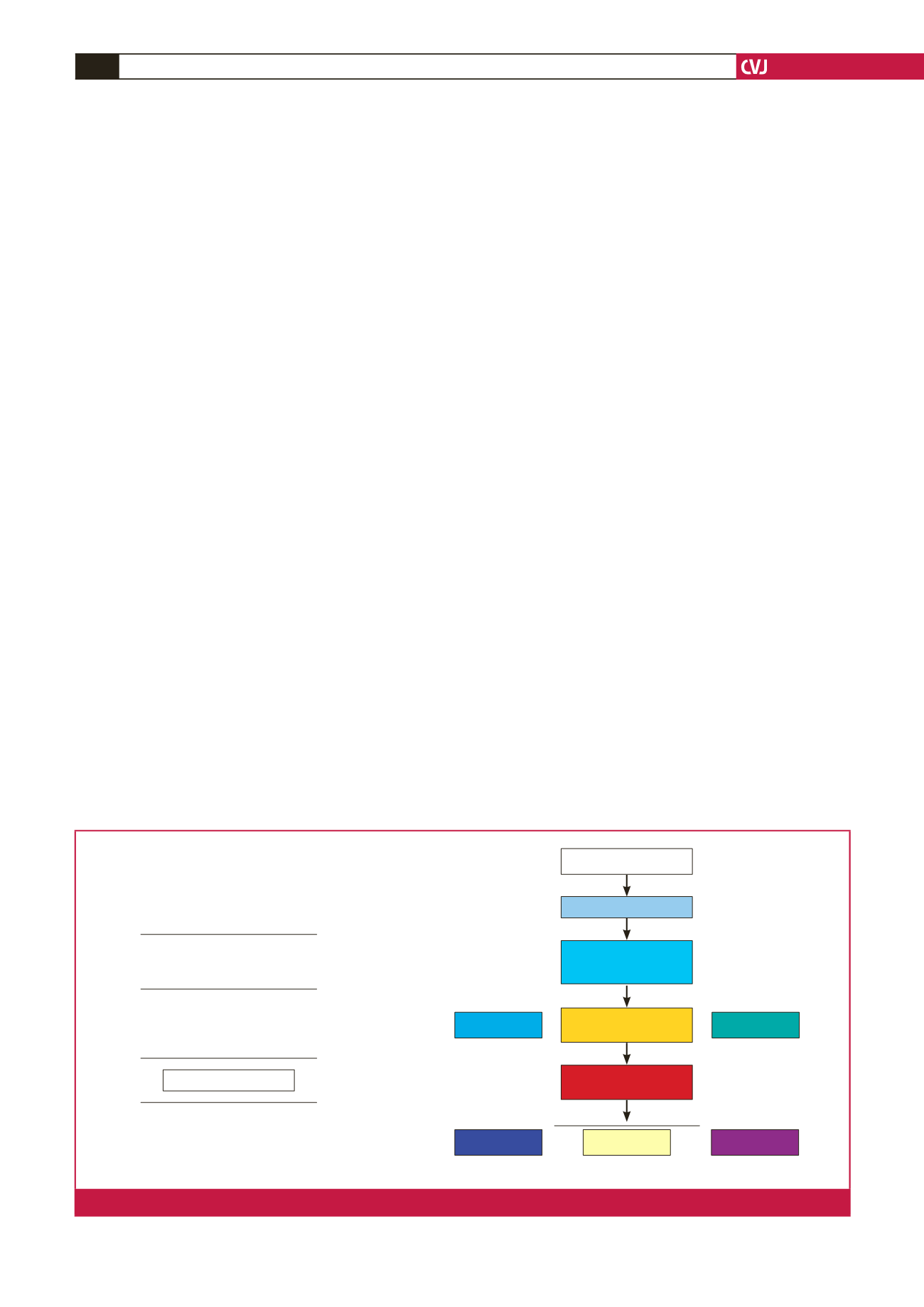
Severe FH patients
Bile acid sequestrant
PCSK9 inhibitor
Statin
? Niacin
? Fibrate
Apheresis
Mipomersen
Lomitapide
Cholesterol-absorption
inhibitor
Initiation of high-intensity statin
monotherapy is standard of care
Ezetimibe is added when patient
is not at LDL-C threshold
Bile acid sequestrants, ? fibrates and
niacin care are added alone or in
combination for those not at LDL threshold
Apheresis for patients on maximally
tolerated therapy and LDL-C > 7.8 mmol/l
or CAD LDL-C > 5.2 mmol/l.
Mipomersen and lomitapide for HoFH
Add a PCSK9 inhibitor
Fig. 4.
Treatment strategies for FH.