CARDIOVASCULAR JOURNAL OF AFRICA • Vol 21, No 4, July/August 2010
202
AFRICA
population are summarised in Table 1.
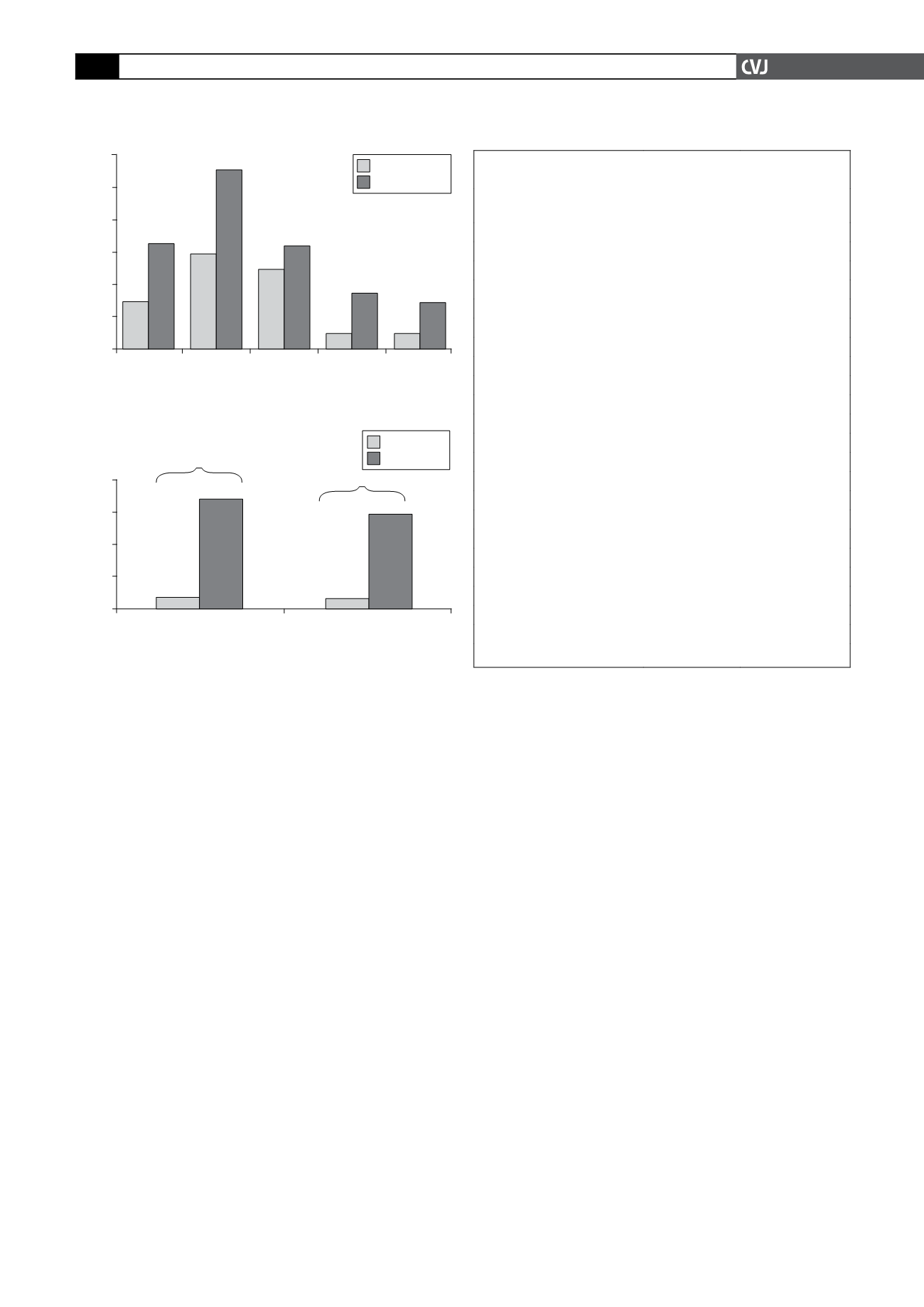
According to Moroccan physicians, MAU is routinely meas-
ured in 35% (95% CI: 22–51%) of their practices versus
37% (95% CI: 35–40%) globally. When asked to estimate the
frequency of MAU in hypertensive patients, 14.6% of physicians
estimated it between 11 and 20% (27.6% globally). However,
61% of the physicians did not provide an estimation of preva-
lence of MAU (Fig. 1).
On the other hand, presence of MAU seemed to influence
97.4% of treatment decisions and particularly those relating to
treatment of blood pressure (100%). Furthermore, 86.1% of
physicians said that MAU also influenced decisions related to
achieving glycaemic control. While the majority (95.12%) of
physicians linked presence of MAU to a patient’s prognosis, all
of them (100%) also felt that a diagnosis of MAU was relevant to
improving the management of other cardiovascular risk factors.
These attitudes were largely comparable with their colleagues
worldwide.
Within the primary analysis of the Moroccan population, few
patients had impaired renal function and 7.5% had previously
known albuminuria. However, urinalysis with a once-off dipstick
test revealed that 67.8% of the study population had evidence of
MAU (58.4%, globally), with prevalence rates slightly higher in
men (69.0%) than women (67.0%) (Fig. 2)
.
Correlations between several cardiovascular risk factors and
MAU were tested in the global study. The following factors
appeared to be associated with presence of MAU: male gender,
large waist circumference, SBP
≥
120 mmHg, DBP
≥
100 mmHg,
creatinine clearance
≥
50 ml/min, and the presence of diabetes,
congestive heart failure, coronary artery disease (CAD), history
of cerebral pathology, peripheral artery disease (PAD), dyspnoea
or palpitations. On the other hand, MAU occurred less often in
patients who had regular physical activity (
<
4 h/week).
Table 2 summarises the prevalence of MAU when associated
with theseparameters in theMoroccanpopulation in this study.The
number of cardiovascular risk factors and cardiovascular diseases
associated with the presence of MAU are shown in Figs 3 and 4.
Use of antihypertensive pharmacotherapy was more frequent
in patients with the presence of MAU. Therefore CCBs (29
vs 21%), ACE inhibitors (32 vs 27%), thiazide diuretics (37
vs 31%) and beta-blockers (43 vs 42%) were more frequently
prescribed in patients with MAU compared to patients without
MAU. However patients with MAU received ARBs less often
(23%) compared to patients without (25%).
Overall, the pharmacotherapy prescribed to patients with
MAU was in the following order: beta-blocker
>
thiazide diuret-
ics
>
ACE inhibitors
>
CCBs
>
ARBs (Fig. 5). The difference
between prescriptions for CCBs and ARBs was significant.
Discussion
The demographic characteristics of the present sample indi-
cated that hypertensive high-risk patients are common in clinical
cardiology. The population was mostly elderly with a substantial
cardiovascular risk-factor profile and a considerable burden of
co-morbidity. Therefore, microalbuminuria is not only a risk
marker for diabetic nephropathy but also indicates a considerable
increase in cardiovascular risk. The investigation of the interde-
pendence of cardiovascular risk and microalbuminuria was of
particular value in this patient population.
TABLE 2. PREVALENCE OF MAUWHENASSOCIATED
WITHTHESE PARAMETERS
Risk factors
Number of
patients
MAU prevalence
(%)
Gender:
male
184
69.02 (61.0–75.3)
female
273
67.03 (61.3–72.3)
Waist circumference:
high
290
72.41 (67.0–77.2)
normal
160
59.38 (51.6–66.7)
Blood pressure: (mmHg)
SBP:
≥
180
138
72.46 (64.5–79.2)
120–129
38
65.79 (49.9–78.8)
DBP:
≥
110
49
71.43 (57.6–82.2)
80–84
113
69.03 (60.0–76.8)
Pulse pressure: (mmHg)
>
80
100
66 (56.3–74.5)
51–60
108
63.89 (54.5–72.3)
Triglycerides:
high (
≥
1.69 mmol/l)
73
73.97 (62.9–82.7)
low (
<
1.69 mmol/l)
101
61.39 (51.6–70.3)
Diabetes:
diabetes (
+
)
87
68.97 (58.6–77.7)
diabetes (–)
368
67.39 (62.4–72.0)
Regular physical activity:
yes
81
62.96 (52.1–72.7)
no
376
68.88 (64.0–73.4)
Fig. 1. Physician-estimated prevalence of MAU.
30
25
20
15
10
5
0
<
10% 11–20% 21–30% 31–40%
>
40%
Morocco
International
% of physicians
Estimated prevalence of MAU
7.32%
16.20%
14.63%
27.60%
12.20%
15.80%
2.44%
8.50%
2.44%
7.20%
Fig. 2. Prevalence of diagnosed and undiagnosed MAU.
80
60
40
20
0
Morocco
Global
known
diagnosed
% of patients
Estimated prevalence of MAU
7.5%
60.3%
6.71%
51.7%
67.8%
60.3%
58.4%


