CARDIOVASCULAR JOURNAL OF AFRICA • Volume 25, No 2, March/April 2014
AFRICA
e3
at the apical thin point, but the fat provided no grip for a catheter.
Therefore, it is not surprising that the catheter easily penetrated
the ventricular wall at the apex. The extremely thin strands of
myocardial muscle at this site are unlikely to withstand the
pressure generated within that chamber during systole.
The whorled arrangement of the muscle fibres
6
allows the
narrow funnel to close off at the onset of systole, so that if the
left ventricular apical thin part has an incomplete perforation,
it is protected from the high pressure generated at the peak of
contraction. In addition, our patient presented with transient
ST-segment elevation in leads V
1
to V
3
following the catheter
penetrating the left ventricular apex, which was probably
associated with acute myocardial injury at the antero-apical
region or vasospasm of the distal left anterior descending artery.
7,8
This possibility is supported by the following aspects.
First, according to fluoroscopy, the location of perforation of
the ventricle was the antero-apical region near the anterior
interventricular groove within which the left anterior descending
artery runs. Second, previous studies
8
have shown that
ST-segment elevation or a Q wave in leads V
1
to V
3
is correlated
with an antero-apical infarct instead of the traditionally termed
anteroseptal acute myocardial infarction, and that the culprit
narrowing is more frequently found in the mid to distal left
anterior descending artery.
Conclusion
Our case highlights the importance of promptly recognising
cardiac perforation. The detection of subtle changes in electrode
potentials and performing angiography via an externally irrigated
ablation catheter lumen may be useful for rapid diagnosis.
References
1.
Friedrich SP, Berman AD, Baim DS, Diver DJ. Myocardial perforation
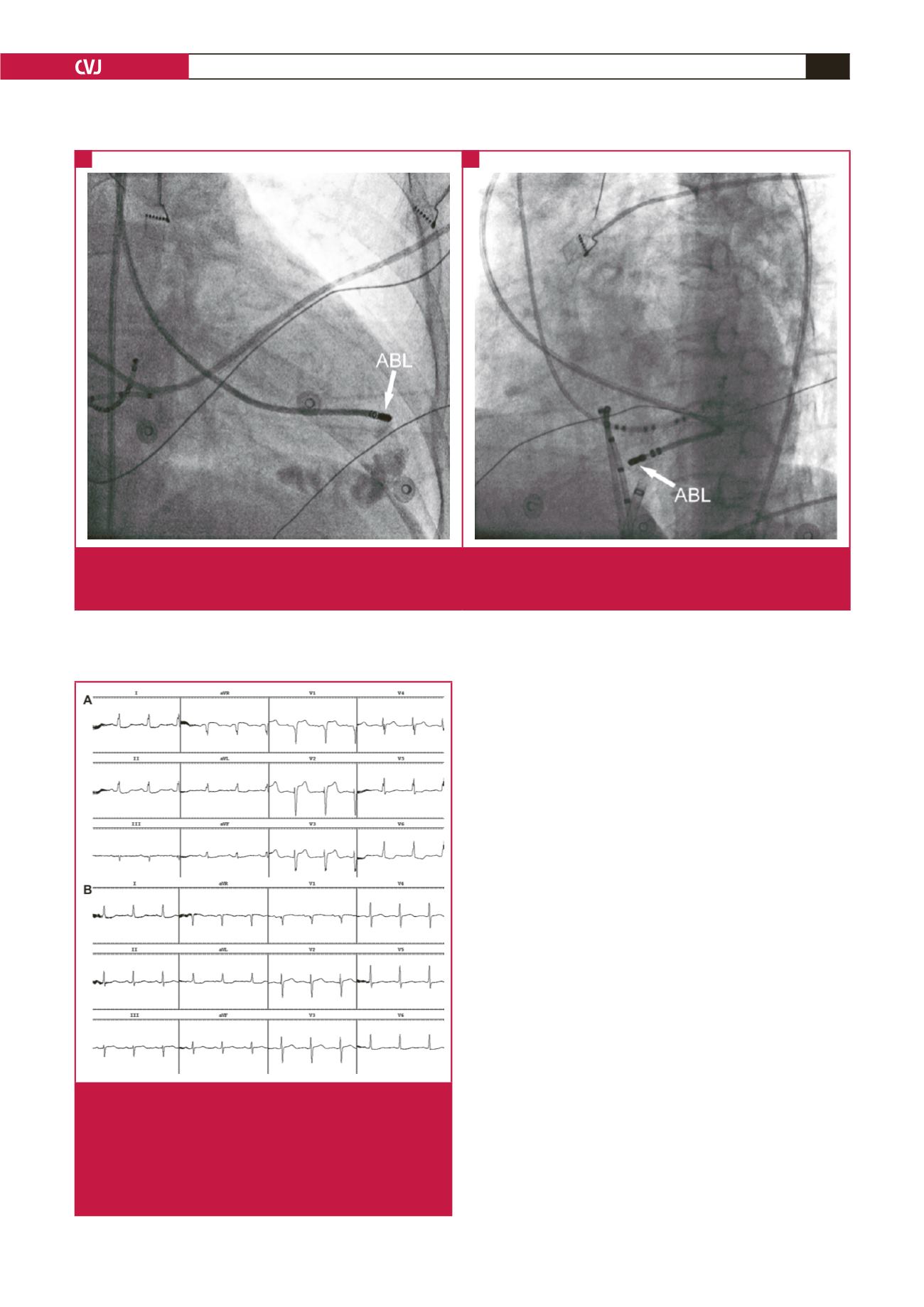
Fig. 3.
Fluoroscopic images of the site of the catheter that had perforated the left ventricle. (A, B) RAO and LAO projections show-
ing the site of the catheter during injection of contrast agent via the ablation catheter lumen and just before injection. ABL
= ablation.
A
B
Fig. 4. Electrocardiogram recording of transient
ST-segment elevation in leads V
1
to V
3
. (A)
ST-segment elevation in leads V
1
to V
3
following
the catheter penetrating the left ventricular apex.
(B) The elevated ST segment in leads V
1
to V
3
was decreased to normal after approximately 20
minutes.


