
















 12 / 70
12 / 70

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 27, No 5, September/October 2016
282
AFRICA
Clinical and laboratory assessments
The patients’ demographic and clinical characteristics were
reviewed using electronic records. The following were extracted:
age, gender, waist and hip circumference, height, weight, history
of diabetes, hypertension and dyslipidaemia. Each patient’s body
mass index (BMI) was calculated, and obesity was defined as
BMI
>
30 kg/m
2
.
13
The waist-to-hip ratio was calculated.
The following laboratory data were extracted: fasting glucose,
haemoglobin (Hb) A
1c
, homocysteine, apolipoprotein A-1, apo-
lipoprotein B, total cholesterol, triglycerides, low-density
lipoprotein cholesterol (LDL-C), high-density lipoprotein
cholesterol (HDL-C), aspartate aminotransferase (AST), alanine
aminotransferase (ALT), gamma-glutamyl transpeptidase
(GGT) and alkaline phosphatase levels.
Carotid ultrasound
CIMT measurements of both common carotid arteries were
performed using a high-resolution ultrasonography Vivid
E9 ultrasound system (GE Healthcare, Little Chalfont, UK)
equipped with an 11-l linear transducer. Far-wall mean CIMT
measurements of longitudinal images were performed at end
diastole in a 10-mm segment located 10 mm proximal to
the carotid bulb. Only plaque-free segments of the common
carotid arteries were used for CIMT analysis. An experienced
ultrasonographer used semi-automated edge-detection software
to calculate the mean CIMT value from a single CIMT
measurement from the left and a single one from the right
common carotid artery, and then averaged the values of the left
and right sides.
Carotid plaque was identified as a focal increase in the
CIMT of greater than 15 mm or greater than 50% of the
surrounding wall.
14
Both common carotid arteries, the carotid
bifurcations, and internal and external carotid arteries were
evaluated for plaque. We defined subclinical atherosclerosis as
a CIMT value higher than the 75th percentile or the presence
of carotid plaque.
Abdominal ultrasound
Abdominal ultrasound was performed by a different experienced
ultrasonographer using an Acuson Sequoia 512 ultrasound system
(Siemens Medical Solutions, USA) equipped with a 4-C1 curved
transducer. Fatty liver disease (fatty infiltration of the liver)
was diagnosed on ultrasound if the liver showed diffuse hyper-
echogenicity relative to the cortex of the right kidney.
15
Normal
hepatic parenchymal echogenicity was considered to be equivalent
to the echogenicity of the cortex of the right kidney.
16
The study
patients were divided into those with fatty liver disease and those
with normal livers, based on the ultrasonographic findings.
Statistical analysis
All categorical data were summarised as frequencies and
percentages, and continuous variables are presented as means
and standard deviations. The Pearson chi-squared test was used
for comparison of categorical variables, and the Fisher exact test
was used for comparison of categorical variables with 20% or
more of the expected cell frequencies lower than 5. The Student’s
t
-test was used for comparison of continuous variables, and the
Mann–Whitney
U
-test was used for sample sizes lower than 30
in at least one group.
Linear-by-linear association was also used to determine trends
for CIMT and the presence of plaque according to age groups.
Univariate followed by multivariate logistic regression analyses
were performed to evaluate the association between fatty liver
disease and atherosclerosis, with adjustment for individual risk
factors, such as age, BMI, hypertension, waist circumference,
and triglyceride, HDL-C and fasting glucose levels, which
included the components of the metabolic syndrome. A
p
-value
less than 0.05 was considered statistically significant. All data
management and analyses were performed using SPSS v 18.0
(SPSS Inc, Chicago, IL).
Results
A total of 630 men and 491 women (aged 51.7
±
11.5 and 54.5
±
11.2 years, respectively) were included in the analysis. Table 1
shows the baseline characteristics of these patients. The men had
significantly higher values for waist-to-hip ratio (0.9
±
0.1 vs 0.8
±
0.1,
p
<
0.001) and BMI (25.5
±
3.2 vs 24.5
±
3.6 kg/m
2
,
p
<
0.001)
than the women. Systolic and diastolic blood pressures were
also significantly higher in the men, and the men had a higher
prevalence of diabetes and dyslipidaemia than the women. In
addition, the mean fasting glucose levels and liver function test
values (AST, ALT, AST/ALT, GGT) were significantly higher in
the men than women. There were no significant differences in
total cholesterol and LDL-C levels between the men and women,
but the triglyceride level was significantly higher in the men.
A total of 472 of 1 121 (42.1%) patients had fatty liver disease.
A significantly higher proportion of men than women had fatty
liver disease (51.4 vs 30.1%,
p
<
0.001) (Table 2). Fig. 2A shows
the prevalence of fatty liver disease in men and women, stratified
by age. A significantly higher proportion of men than women
aged 60 years and under had fatty liver disease. There was no
difference in the prevalence of fatty liver disease between the
male and female patients aged older than 60 years.
The mean CIMT measurement of men was significantly
higher than that of the women (0.79
±
0.17 vs 0.76
±
0.17 mm,
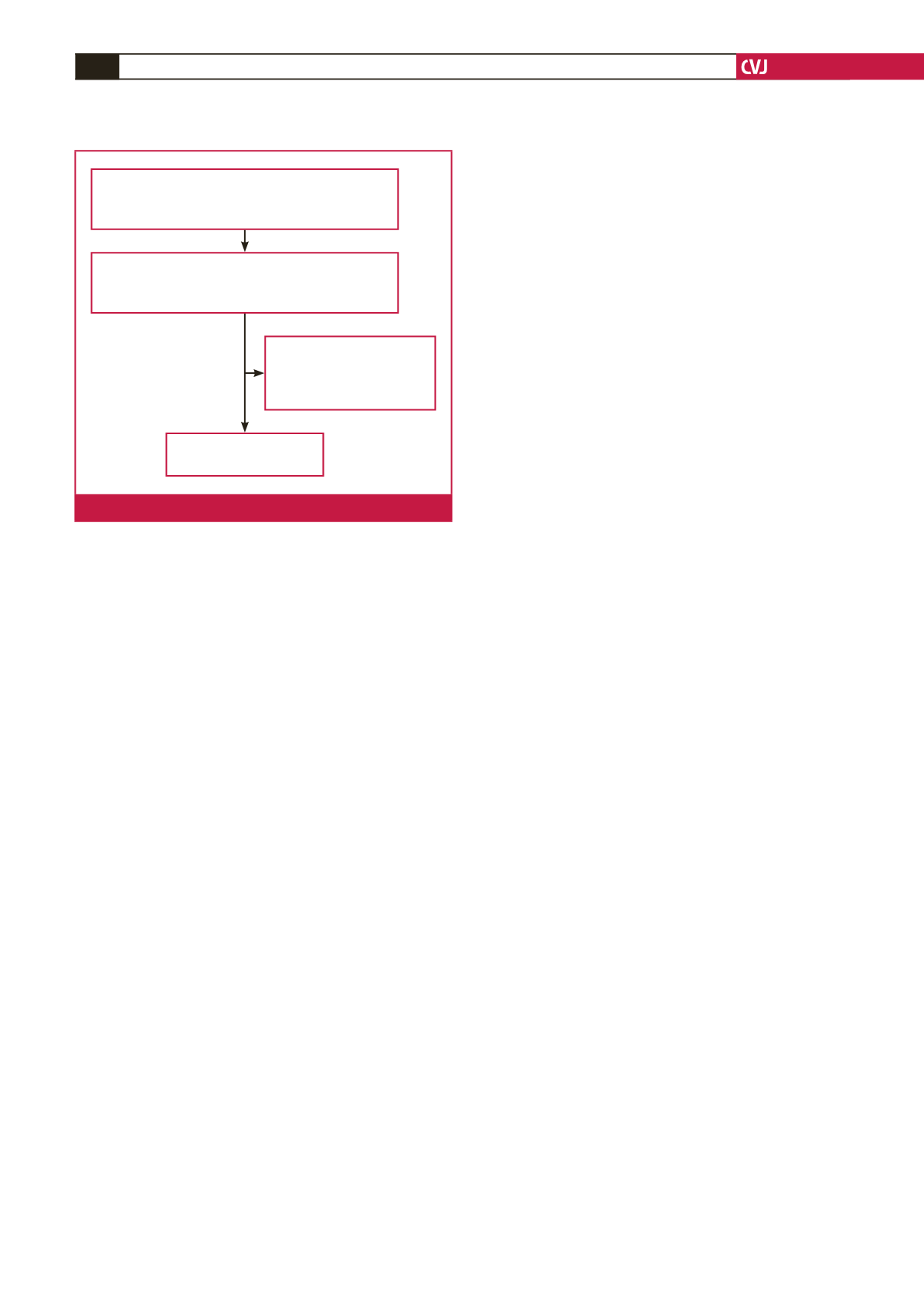
Patients who visited the healthcare centre for
routine check up from June 2011 to December 2013
(
n
=
23 474)
Patients who had carotid and
abdominal ultrasound performed
(
n
=
1 366)
60 with hepatitis B virus
6 with hepatitis C virus
179 with excessive alcohol
consumption (
≥
20 g/day)
Final analysis
(
n
=
1 121)
Fig. 1.
The study population.