


















 57 / 62
57 / 62

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 31, No 4, July/August 2020
AFRICA
219
She began treatment to prevent heart failure and her condition
stabilised after a six-week complicated course of hospitalisation.
She was followed up two months after discharge and was doing
well. Repeat TTE revealed no vegetation on the tricuspid valve
and only mild regurgitation.
Discussion
Right-sided infective endocarditis is an uncommon entity,
accounting for 5 to 10% of all cases of infective endocarditis, and
frequently involves the tricuspid valve.
3
It occurs predominantly
in intravenous drug abusers. In non-drug abusers, predisposing
conditions include congenital heart disease, use of a PICC or
central catheter, and right-sided cardiac instrumentation.
1
The
widespread use of PICCs worldwide has led to an increasing
incidence of right-sided infective endocarditis, which is recognised
as a serious PICC-related complication.
The incidence of infective endocarditis is higher when the
tip of the catheter is deep in the right atrium.
4
The potential
mechanism is that when the tip is deep in the right atrium
or in close proximity to the tricuspid leaflet, abrasion of
the endocardium or tricuspid valve causes endothelial injury,
allowing microorganisms to establish infection on the damaged
endocardial surface.
2
Suresh
et al
. reported a case of tricuspid
valve endocarditis secondary to injury by a central venous
catheter and found a large vegetation extending down the
chordal apparatus during surgery.
2
In our case, the PICC tip floated into the right ventricle
in diastole and injury of the chordae tendinae could not be
excluded because TTE could not reveal tiny vegetations. More
importantly, each time the PICC line returned to the right atrium
in systole, the tip stabbed the tricuspid valve. This was almost
sure to trigger direct injury of the valve. The large vegetation
on the anterior tricuspid leaflet confirmed our hypothesis that
direct injury induced by the tip of the overly long PICC line was
the chief cause of the endocarditis. Perforation of the tricuspid
leaflet was also possible because the tip stabbed the valve
constantly and the tricuspid regurgitation was more severe than
at the end of chemotherapy three months previously. Therefore,
accurate localisation of the PICC tip is extremely important as
the first and most important step of infection control.
Although optimal tip location is controversial, most guidelines
recommend localisation in the lower one-third of the superior
vena cava to the superior vena cava/right atrial junction. The
major issue in PICC placement is how to determine the catheter
length or tip position. Various anthropometric measurement
techniques have been described. In one report, for instance,
the insertion length was evaluated by measuring the distance
Fig. 2.
Postero-anterior chest radiograph demonstrating the
tip location (white arrow) of the PICC line near the
superior cavo-atrial junction.
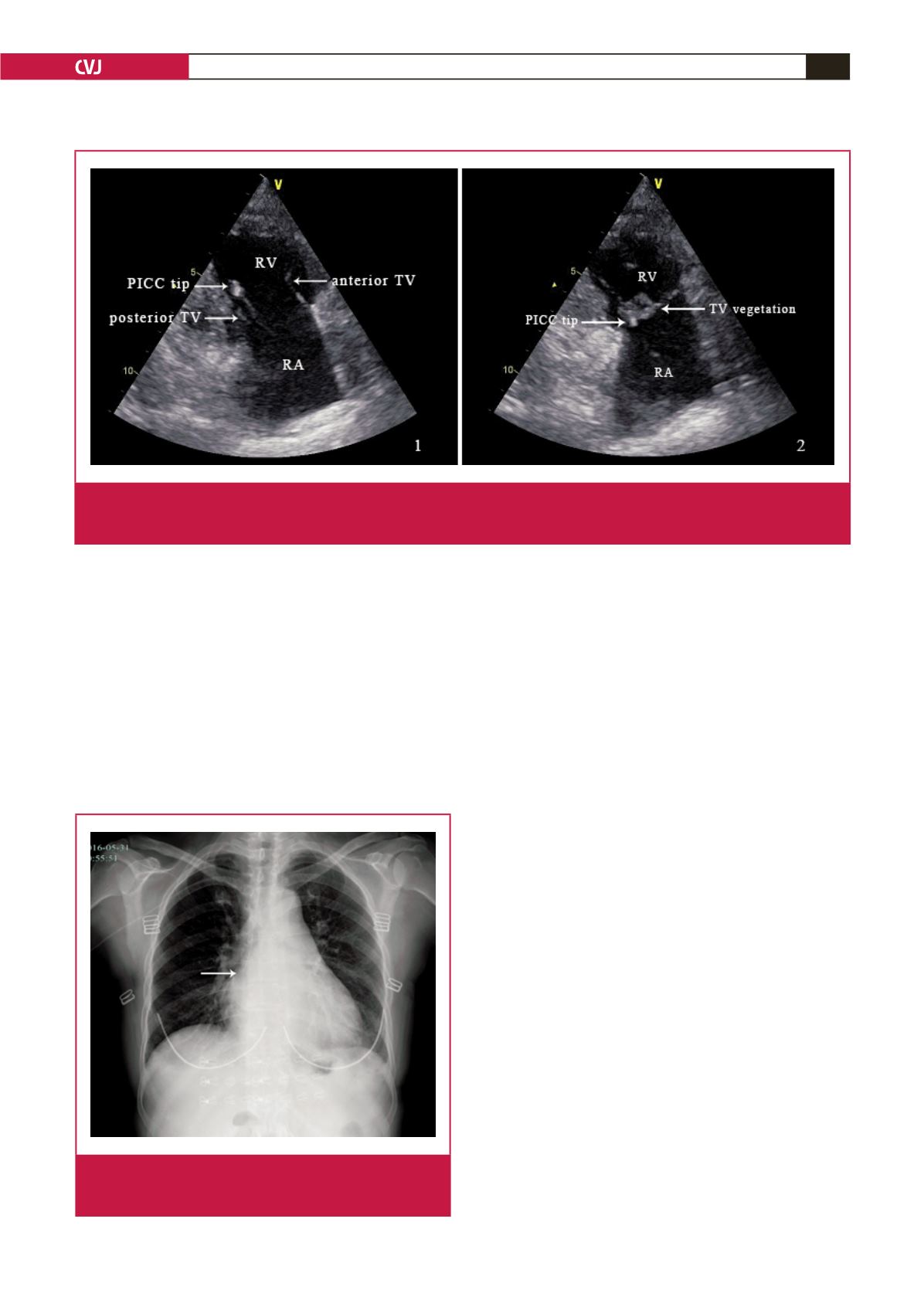
Fig. 1.
The PICC line on TTE image. 1. TTE showing a small echodensity on the tip of the PICC line, which is in the right ventricle
in diastole. 2. TTE showing a large vegetation on the anterior tricuspid leaflet and the PICC tip stabbing the valve in systole.
RV, right ventricle; RA, right atrium; TV, tricuspid valve.