CARDIOVASCULAR JOURNAL OF AFRICA • Vol 23, No 2, March 2012
AFRICA
95
opment of insulin resistance and other metabolic abnormalities.
28
This could be one of the explanations for the presence of HHD
in our study. However, because increasing age was independently
associated with the outcome of HHD in our patients, it is possi-
ble that the usual cardiovascular risk factors had a role to play, as
has been reported by other investigators.
29,30
In this study, higher haemoglobin level was independently
associated with the diagnosis of HHD. This was an unexpected
finding, but the explanation could be that HIV-infected patients
with HHD were generally less sick compared to the rest of the
study patients without HHD and therefore had significantly
better haemoglobin levels. It should be emphasised however that
the average haemoglobin level in the patients with HHD (11.8 g/
dl) was slightly lower than normal.
The incidence of HIV-associated pulmonary hypertension is
estimated to be 1/200; much higher than the 1/200 000 found
in the general population.
31
In our cohort, pulmonary hyperten-
sion was present in 13% of the patients. Niakara
et al
. found the
prevalence of pulmonary hypertension to be 5% in HIV-infected
patients hospitalised in a cardiac unit in Harare.
32
The difference
between our study and that of Niakara could be that his study was
retrospective and some cases of pulmonary hypertension could
have been missed because no clear definition was set before-
hand. Our cohort included out-patients, therefore increasing the
chances of having more cases with pulmonary hypertension.
The usual presentation of patients with pulmonary hyper-
tension is shortness of breath, and in most cases this is attrib-
uted to lung disease. These patients generally appear to have no
advanced immunosuppression, in other words no relation to the
disease stage as reflected by CD
4
count.
33
The majority of our
patients presented with shortness of breath, which was out of
proportion to the physical findings, and the average CD
4
count
was 242
±
208 cells/µl. This is similar to that reported by Le
Houssine
et al
.
34
in their analysis of nine HIV-infected patients
with primary pulmonary hypertension, in which the mean CD
4
count was 234
±
217cells/
µ
l.
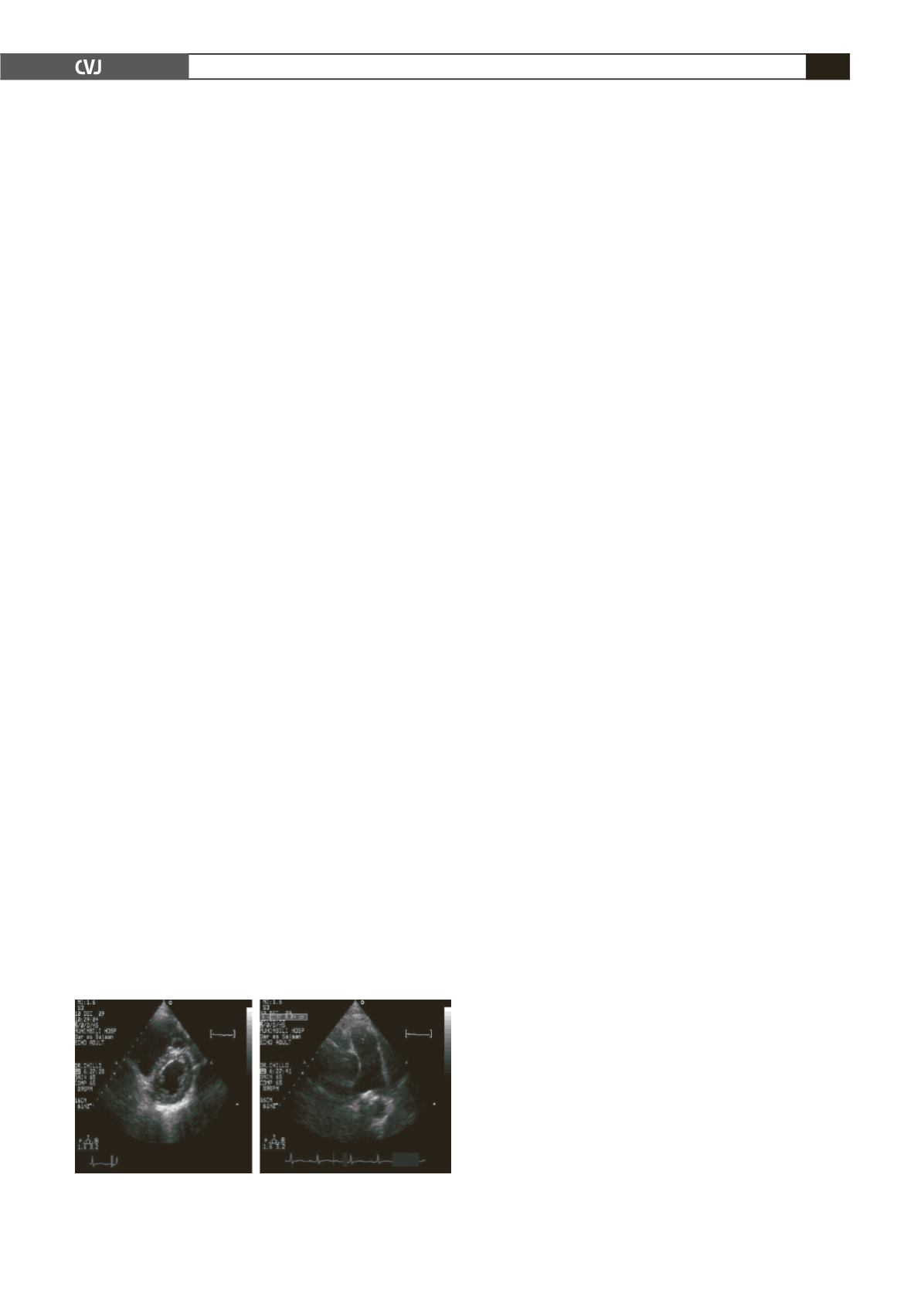
In multivariate analysis, we found no single predictor of
pulmonary hypertension. The echocardiographic findings were
those of dilated right heart with a prominent D-sign on paraster-
nal short-axis view. Often the main pulmonary artery was also
dilated (Fig. 1). The prognosis of these patients is generally poor,
with median survival of approximately six months.
33
Dilated cardiomyopathy is probably the most studied form of
heart muscle disease in HIV-infected patients. The prevalence of
dilated cardiomyopathy has been reported to be up to 40%, with
an annual rate of incidence of 15.9 cases per 1 000 patients.
35
The
condition is generally associated with advanced immunosuppres-
sion and poor outcome.
36
We found 10 cases (9.8%) of dilated cardiomyopathy in a
seven-month period. All 10 patients were in heart failure and
with advanced immunosuppression, with an average CD
4
cell
count of 83 cells/
µ
l. These patients were generally young with a
mean age 35 years and short duration after HIV diagnosis. Often
the first presentation to hospital was heart failure.
The formation of dilated cardiomyopathy is thought to be due
to either the direct action of HIV on the myocardial tissue or to
an autoimmune process induced by HIV, possibly in association
with other cardiotropic viruses.
37
Poor nutritional status has also
been implicated and may be a greater role player in sub-Saharan
Africa where idiopathic dilated cardiomyopathy is also preva-
lent.
38
Nutritional deficiencies are common in HIV infection,
particularly in late stages of the disease and may be due to poor
absorption of food and prolonged diarrhoea.
39
Deficiency of
trace elements such as selenium have also been directly or indi-
rectly associated with cardiomyopathy.
40,41
The finding of two cases of aneurismal dilatation of the aorta
in our study is not unique. This pathology has been reported by
other investigators.
42,43
These case reports describe aneurysms
of the aorta and peripheral cerebrovascular arteries, sometimes
necessitating surgical repair. The aneurysms are probably a result
of vasculitic changes induced by the virus, or by other infectious
causes such as cytomegalovirus and tuberculosis.
44
However, an
infective agent was not always identified.
44
The inclusion in our study of patients with palpitations could
have resulted in over-inclusiveness, because palpitation as a
symptom is non-specific. However, most patients had palpita-
tions plus other cardiac symptoms, since the majority of our
patients had more than one symptom. In fact, palpitations was a
symptom in 91% of the patients.
The majority of patients in this cohort had anaemia, which
is often accompanied by palpitations. Unless heart failure has
occurred, the echocardiographic findings in these patients would
most likely be normal. This could explain the 18 patients in our
study who had a normal echocardiograph. Shortness of breath
is a symptom of lung disease and if these patients were also
anaemic and had tachycardia, it would be easy to surmise they
had a cardiac condition, further explaining the normal echocar-
diographs.
We acknowledge several limitations of this study. First,
although this study was powered to detect differences in cardiac
involvement between patients with different immunological
status, the same was not true for other factors that may also have
contributed to the development of specific cardiac conditions,
such as alcohol consumption and cigarette smoking. This could
have resulted in the lack of association.
Second, this study did not include viral load and socio-
economic status, which are important predictors of dilated
cardiomyopathy, as reported by Twagirumukiza and co-workers.
9
Third, as is the case for all cross-sectional studies, a causal
relationship cannot be claimed and therefore the findings of this
study should be interpreted with caution, as it is not possible to tell
whether HIV infection resulted in cardiac disease or vice versa.
Conclusion
The pattern of cardiac abnormalities in this era of HAART is still
dominated by pericardial disease and cardiomyopathy, as seen in
Fig. 1. D-sign (left image) and dilated main pulmonary
artery (right image) in a patient with pulmonary hyperten-
sion.


