CARDIOVASCULAR JOURNAL OF AFRICA • Vol 23, No 2, March 2012
AFRICA
105
tration however on CVD constituents and major risk factors such
as hypertension and diabetes mellitus. Baseline evaluation also
included either risk factors or status for specific cardiovascular
diseases (Table 1). Outcomes monitored in general had a focus
on mortality and trajectories of risk markers. The capacity of
these studies for retaining participants during follow up showed
some heterogeneity not explained by the duration of follow up or
time period of the study (Table 2).
Cohort with a focus on mortality at baseline or
during follow up
Stroke
: five hospital studies have followed individuals in the post-
stroke period for mortality and disabilities.
24,44,46,58,61,62
Collectively,
these studies have provided follow-up information on about 1
244 individuals over a period of six months to four years.
Heart failure
: two studies in Nigeria monitored the outcomes
of patients with specific types of heart failure: hypertensive and
peripartum heart failure. Izuezo and his colleagues
52
monitored a
cohort of 107 patients with hypertensive heart failure for mortal-
ity over a 12-month duration. The rate of death was 29%, and
22% of these deaths were recorded within the first three months
of follow up. Predictors of death included the duration of diag-
nosed heart failure, blood pressure variables, age, baseline serum
creatinine, and treatment with captopril.
Parry and his collaborators
23,28,53-55
followed for more than 20
years a cohort of 227 women with peripartum heart failure at
baseline in Zaria. The mortality rate in this study was 11% within
two to five years of follow up, and 42% at 20 years; the major-
ity being cardiovascular. Predictors of death and changes in the
status of heart failure were investigated. However, the techniques
used for such analysis failed to accommodate the varying time
of occurrence of event between participants, and was unable
to provide information beyond differences in the mean levels
or prevalence of predictors between subgroups of participants.
Parry and his colleagues also described the changing trends of
blood pressure variables and the incidence of hypertension in
the cohort.
Rheumatic heart disease, cardiac infections
: three cohort stud-
ies with a focus on rheumatic heart disease were identified. A
group of 75 patients with acute rheumatic fever was monitored
in Zimbabwe for about 12 years for incident cardiac complica-
tions and deaths.
106
The average time to development of chronic
valvular disease and heart failure was 2.8 and 5.2 years, respec-
tively, and death was likely to occur in young patients at baseline.
Fadahunsi
26
in Nigeria reported on a cohort of 92 patients with
established rheumatic heart disease from the time of their first
hospital contact. Retention of participants was low, with only
one-third of participants still regularly attending visits after 10
years into the study.
In 1972, a clinical screening was conducted on 12 050
schoolchildren in Soweto, during which 168 children had auscul-
tation signs suggestive of rheumatic valvular disease.
22
Four
years later, 139 of these children were traced and re-examined
to monitor changes in their heart sounds in the absence of
prophylaxis against rheumatic activity. This re-examination
revealed that most of the auscultation abnormalities identified
during the first examination were not features of rheumatic
heart disease. However, recently, asymptomatic patients without
cardiac murmur were found to have echocardiographic abnor-
malities that were suggestive of rheumatic heart disease.
107
The
clinical and prognostic significance of clinically silent echocar-
diographic abnormalities of suspected rheumatic heart disease
needs to be determined in prospective randomised studies of
penicillin prophylaxis.
Two cohort studies followed patients in relation to cardiac
infections in SSA. From 1997 to 2000, Koegelenberg in South
Africa investigated and followed patients referred for presump-
tive infective endocarditis.
32
Of the 92 examined at baseline, 35%
had a diagnosis other than infective endocarditis. Seventy-three
per cent of those with infective endocarditis had a history or
echocardiographic features of rheumatic heart disease. Eighty-
one per cent of those without infective endocarditis had under-
lying rheumatic heart disease. The six-month crude mortality
rate was 35.6% in those with a confirmed diagnosis of infective
endocarditis, and 12.9% among those without.
Between March and October 2004, a cohort of 185 patients
with presumptive pericardial tuberculosis was established from
15 referral hospitals in Cameroon, Nigeria and South Africa.
37
These patients were observed for a six-month period under
specific treatment for major outcomes, including mortality. The
overall mortality rate was 26% among 174 patients, with infor-
mation available on their vital status at the study completion.
Using Cox regression models, independent predictors of death
during follow up were: a proven non-tuberculosis final diagno-
sis, the presence of clinical signs of HIV infection, coexistent
pulmonary tuberculosis, and older age.
37
Among survivors, clini-
cal signs of HIV infection at baseline were associated with lower
risk of developing a pericardial constriction during follow up.
108
Multiple outcomes:
we identified one community-based inter-
vention study, the Coronary Risk Factor Study (CORIS). This
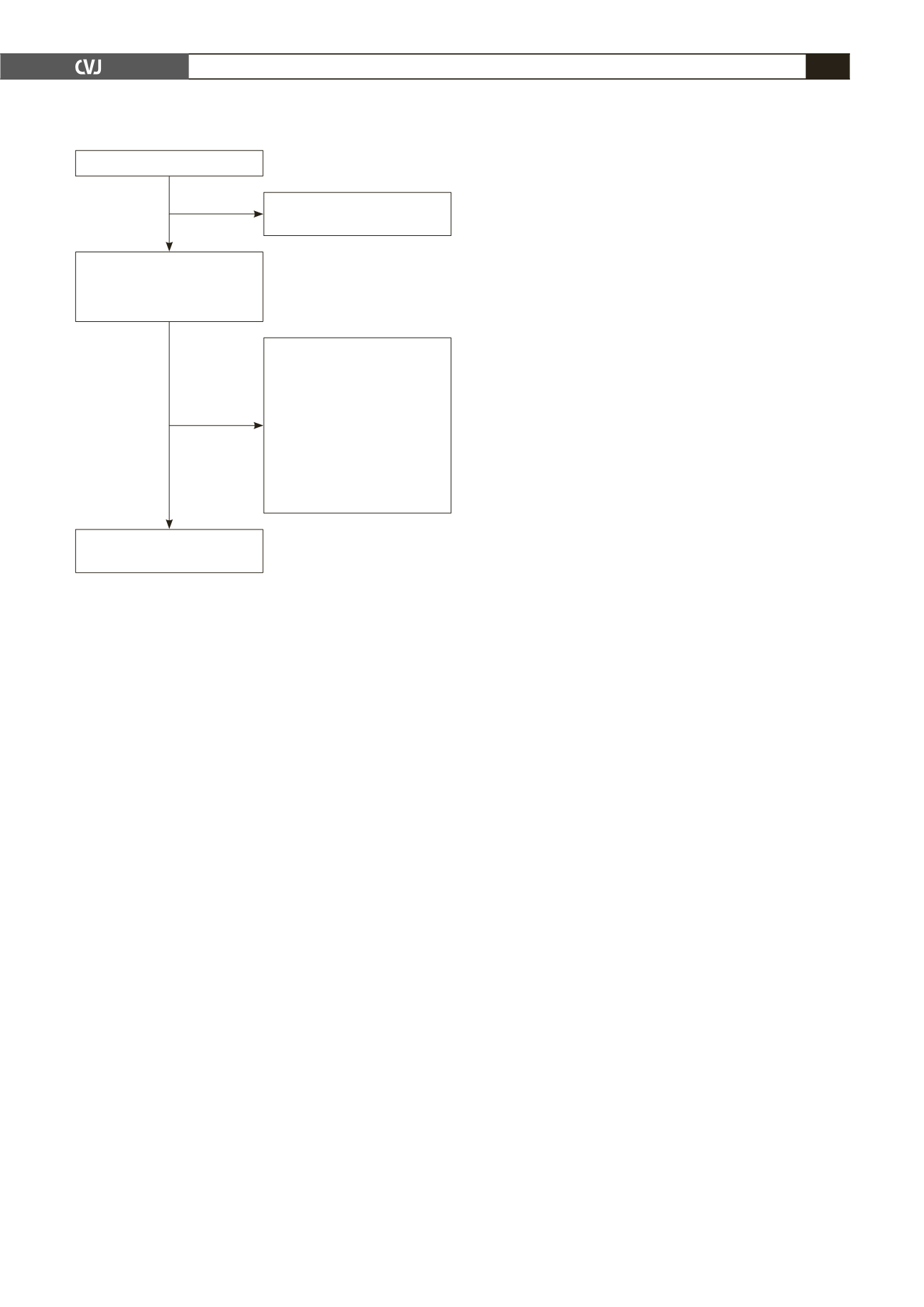
Articles extracted: 788
676 articles excluded (not
meeting the inclusion criteria)
112 articles potentially
relevant
Inclusion assessment by
abstract/full text
13 cross-sectional studies
9 studies: no abstract
available
4 studies: short duration of
follow up (< 6 months)
3 migrant studies
1 small sample (< 30
participants)
1 surveillance study
Articles included in the
review: 81
Fig. 1. Flow chart of studies in the review.


