CARDIOVASCULAR JOURNAL OF AFRICA • Vol 24, No 3, April 2013
e2
AFRICA
Patients with LVNC may be asymptomatic or present with
cardiac dysfunction, ventricular arrhythmias or systemic emboli.
3
In this report we present a patient diagnosed with LVNC during
pregnancy. Despite being congenital, the reason for this patient
becoming symptomatic may be explained by the haemodynamic
changes during the pregnancy.
During pregnancy, blood volume and cardiac output increase,
which may precipitate symptoms of heart failure.
8
Although
maximal haemodynamic changes occur earlier in pregnancy,
7
the
patient had attributed her symptoms solely to pregnancy, until
she became frankly dyspnoeic. Indeed, symptoms of heart failure
such as dyspnoea, dizziness, pedal oedema, and orthopnoea
can occur even in normal pregnancies.
8
Nevertheless, if the
symptoms develop suddenly or become serious, as in this case,
further evaluation is needed.
Traditionally, left ventricular non-compaction is diagnosed
by two-dimensional and colour Doppler echocardiography.
A number of echocardiographic definitions for the diagnosis
of LVNC are used. Commonly used criteria include the
identification of excessive (more than three) prominent (more
than 2 mm in diameter) trabeculae with inter-trabecular recesses
that penetrate deeply into the myocardium, from which blood
flows directly into and out of the ventricular cavity (which is
demonstrated using colour Doppler imaging), in the absence of
other structural heart disease.
9
The method Jenni and colleagues proposed relies on the
detection of two myocardial layers, compact and non-compact,
in short-axis views of the left ventricle in end-systole. LVNC is
diagnosed according to the ratio of these layers.
4,10
Increasingly,
MRI is being used and CT may be of value.
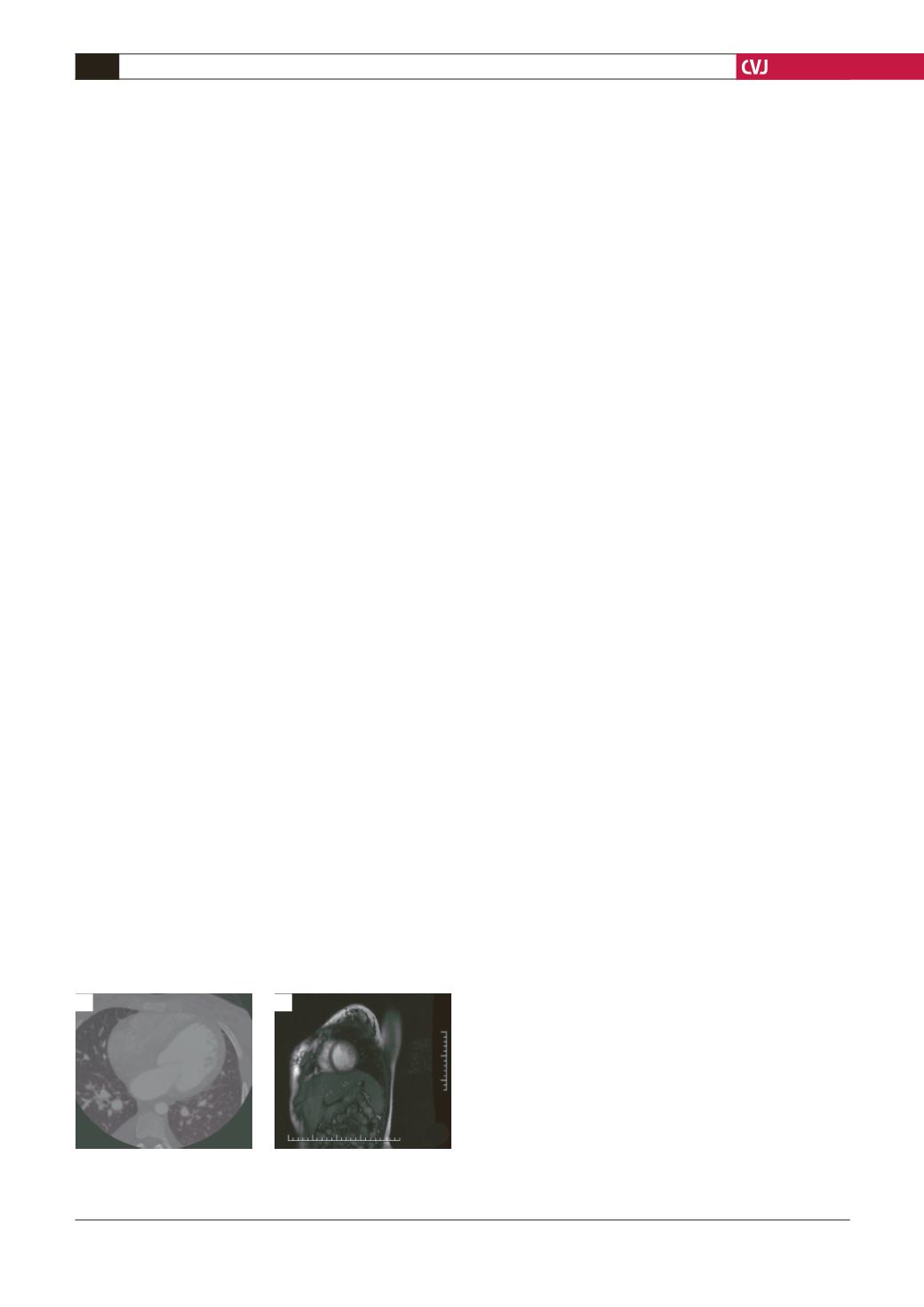
In this case, the diagnosis of LVNC was made by
echocardiography showing excessive prominent trabeculations,
with colour Doppler echocardiography revealing blood flow
between the trabeculations. Trabeculation was predominant
in the apex and the lateral wall and this was consistent with
previous work by Boyd
et al
.
10
Computed tomography and MRI
revealed similar trabeculations in this patient (Fig. 2).
The differential diagnosis for this patient included peripartum
cardiomyopathy, which is a formof idiopathic primarymyocardial
disease associated with pregnancy. The European Society of
Cardiology recently defined peripartum cardiomyopathy as a
form of dilated cardiomyopathy that presents with signs of heart
failure in the last month of pregnancy or within five months of
delivery.
11
However, in our case it was not possible to determine
whether this clinical presentation was due to LVNC that became
symptomatic with the haemodynamic changes of pregnancy, or
whether peripartum cardiomyopathy complicated this patient’s
pregnancy.
Conditions that may be falsely diagnosed as LVNC should
also be included in the differential diagnosis. These conditions
include false tendons, aberrant bands, thrombi, the apical type of
hypertrophic cardiomyopathy, fibromas, obliterative processes of
the left ventricular cavity, intra-myocardial haematomas, cardiac
metastases, and intra-myocardial abscesses.
12
However, both
imaging modalities showed prominent trabeculations and the
patient’s clinical course made these diagnoses unlikely.
Conclusion
Dyspnoea is common during pregnancy. Development of
dyspnoea in the pregnant woman leaves the clinician with the
question of whether the dyspnoea comes from an underlying
cardiac or pulmonary disease or it is due to the pregnancy itself.
This case reminds us that although LVNC is rarely diagnosed
in pregnancy, rare causes of heart failure should also be kept in
mind during the evaluation of symptoms of heart failure.
References
1.
Richardson P, McKenna W, Bristow M, Maisch B, Mautner B,
O’Connell J,
et al.
Report of the 1995 World Health Organization/
International Society and Federation of Cardiology Task Force on the
definition and classification of cardiomyopathies
. Circulation
1996;
93
: 841–842.
2.
Pignatelli RH, McMahon CJ, Dreyer WJ, Denfield SW, Price J, Belmont
JW,
et al.
Clinical characterization of left ventricular noncompaction in
children: a relatively common form of cardiomyopathy.
Circulation
2003;
108
(21): 2672–2678.
3.
Murphy RT, Thaman R, Blanes JG, Thaman R, Blanes JG,
et al.
Natural
history and familial characteristics of isolated left ventricular non-
compaction.
Eur Heart J
2005;
26
: 187–192.
4.
Kohli SK, Pantazis AA, Shah JS, Adeyemi B, Jackson G, McKenna
WJ,
et al
. Diagnosis of left-ventricular non-compaction in patients with
left-ventricular systolic dysfunction: time for a reappraisal of diagnostic
criteria?
Eur Heart J
2008;
29
(1): 89–95.
5.
Bladt O, Vanhoenacker R, Bevernage C, Leyman P. Isolated noncom-
paction of ventricular myocardium. Diagnosis with multidetector
computed tomography.
JBR-BTR
2008;
91
(4): 153–154.
6.
Munehisa Y, Watanabe H, Kosaka T, Kimura A, Ito H. Successful
outcome in a pregnant woman with isolated noncompaction of the left
ventricular myocardium.
Intern Med
2007;
46
(6): 285–289.
7.
Patel C, Shirali G, Pereira N. Left ventricular noncompaction mimick-
ing peripartum cardiomyopathy.
J Am Soc Echocardiogr
2007;
20
(8):
1009.e9
–
12.
8.
Ramaraj R, Sorrell VL.Peripartum cardiomyopathy: Causes, diagnosis,
and treatment.
Cleve Clin J Med
2009;
76
(5): 289
–
96.
9.
Ahmed I, Phan TT, Lipkin GW, Frenneaux M. Ventricular noncompac-
tion in a female patient with nephropathic cystinosis: a case report
. J
Med Case Reports
2009;
29
(3): 31.
10. Boyd MT, Seward JB, Tajik AJ, Edwards WD. Frequency and location
of prominent left ventricular trabeculations at autopsy in 474 normal
human hearts: implications for valuation of mural thrombi by two-
dimensional echocardiography
. Am Coll Cardiol
1987;
9
: J323–326.
11. Elliott P, Andersson B, Arbustini E, Bilinska Z, Cecchi F, Charron P,
et
al.
Classification of the cardiomyopathies: a position statement from
the European Society of Cardiology Working Group on Myocardial and
Pericardial Diseases.
Eur Heart J
2008;
29
(2): 270–276.
12. Stöllberger C
,
Finsterer J. Pitfalls in the diagnosis of left ventricular
hypertrabeculation/non-compaction.
Postgrad Med J
2006;
82
(972):
679
–6
83.
Fig. 2. A: computed tomography. B: magnetic resonance
imaging showing increased trabeculation.
B
A


