CARDIOVASCULAR JOURNAL OF AFRICA • Vol 24, No 3, April 2013
e4
AFRICA
Chest radiography (Fig. 1) demonstrated hypoplasia of the
right lung, with a right mediastinal shift. There were hemi-
vertebrae and a mild scoliosis present.
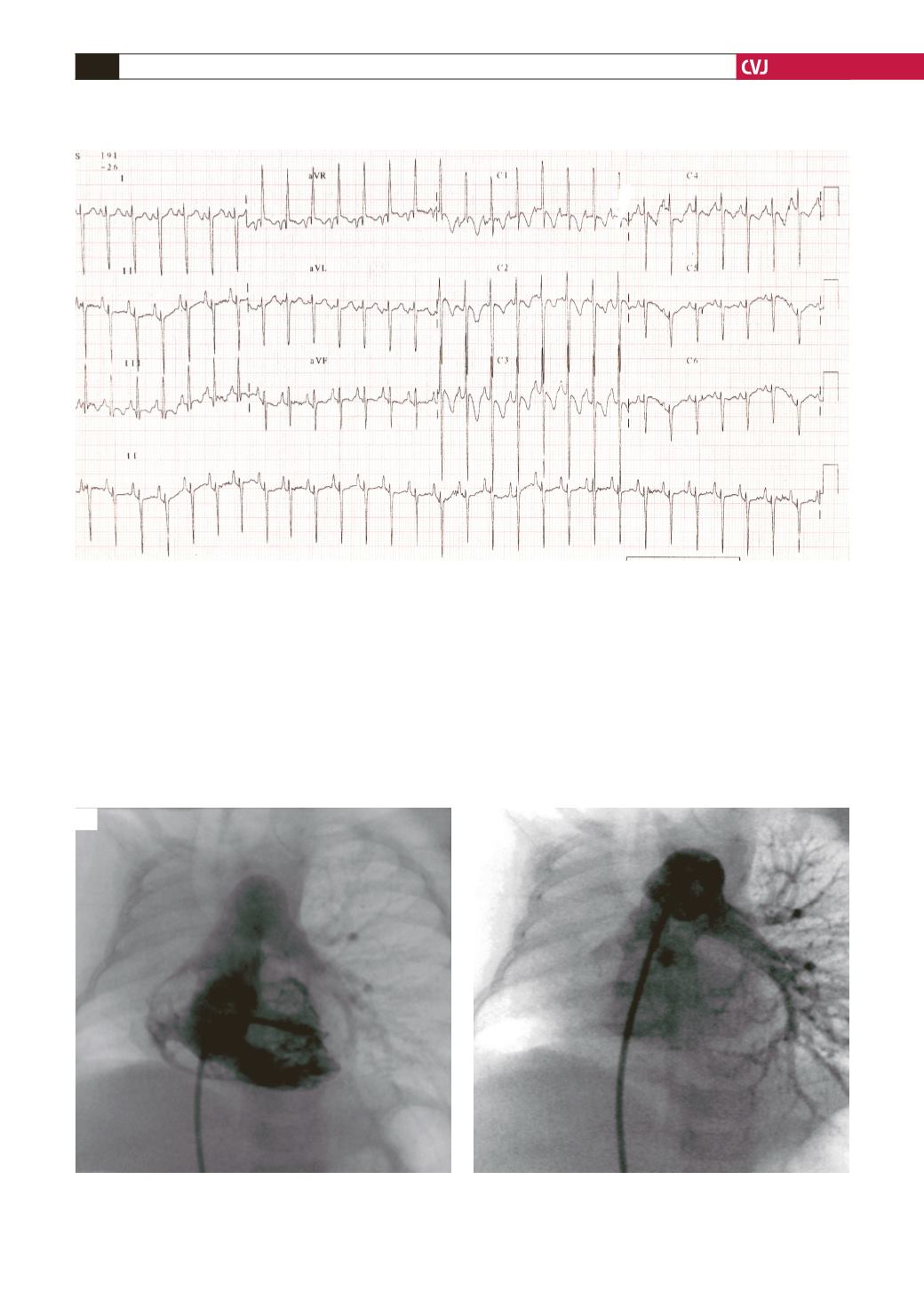
Electrocardiography (Fig. 2) demonstrated a heart rate of 170
beats/min, extreme right-axis deviation, right atrial enlargement
and marked right ventricular hypertrophy. On echocardiography
the heart was shifted over to the right hemithorax and standard
views could be obtained by moving the probe towards the right
chest.
There was situs solitus and no atrial or ventricular inversion.
The right atrium (RA), right ventricle (RV) and main pulmonary
artery (MPA) segment were dilated. The dilated right heart
compressed the left, with both the interventricular and interatrial
septa deviated to the left. The estimated pulmonary pressure
from the tricuspid regurgitation gradient was 70 mmHg. A small
patent foramen ovale with bidirectional shunting was noted. The
right pulmonary artery (RPA) could not be visualised. The left
pulmonary veins drained normally into the left atrium, but the
Fig. 2. Electrocardiogram demonstrates tachycardia, extreme right-axis deviation, right atrial enlargement and right
ventricular hypertrophy.
Fig. 3. RV (A) and MPA (B) angiograms demonstrating RV hypertrophy and an absent RPA. Tracheal deviation to the
right is also shown (arrows). (RV, right ventricle; MPA, main pulmonary artery; LPA, left pulmonary artery; RPA, right
pulmonary artery).
A
B
LPA
LPA
RV
RV


