


















 12 / 74
12 / 74

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 25, No 5, September/October 2014
206
AFRICA
catheterisation laboratory in Uganda at the time of the study).
HF was defined as hypertensive when long-lasting history of
systemic hypertension and typical echocardiographic features
such as left ventricular concentric hypertrophy or impaired left
ventricular inflow patterns were found. We identified patients as
potential candidates for cardiac surgery according to the current
guidelines.
14
This study was approved by the St Raphael of St Francis
Nsambya Hospital Ethical Committee (May 2009). It conformed
to the Declaration of Helsinki and Good Clinical Practice.
Statistical analysis
We performed descriptive statistics for the more frequently
observed heart diseases. The results are reported as median
and interquartile range, or as numbers and percentages, as
appropriate.
Results
Causes of HF in the whole cohort and according to age
The study group constituted a cohort of 140 patients with
clinical HF. Median age was 40 years (IQR 14–66) and 83 (59%)
were female. All patients were black Africans. The predominant
cause of HF was RHD (
n
=
44; 31%) (Fig. 2A), mainly related
to severe mitral regurgitation, which was either isolated or
associated with multiple valve involvement. Other main causes
of HF were CHD (
n
=
41; 29%), hypertensive cardiomyopathy (
n
=
22; 16%), highly suspected IHD (
n
=
14; 10%), endomyocardial
fibrosis (EMF) (
n
=
8; 6%) and right ventricular failure due to
pre-capillary PH (
n
=
7; 5%).
LVEF was reduced in 56 cases (40%). Moderate to severe
right ventricular dysfunction was found in 70 (50%) cases.
Clinical and echocardiographic characteristics of patients with
HF are depicted in Table 1.
We further analysed causes of HF separately in children and
adults (Fig. 2B, C). In the paediatric population [
n
=
50, age
≤
16 years, median 6 (IQR 2–12)] CHD was the main cause of HF
(
n
=
30; 60%), followed by RHD (
n
=
16; 32%). We also reported
three cases of EMF (6%). In the first decade of life, CHD was
the main cause of HF (29/31, 97%), while RHD was the most
prevalent in the age group of 10 to 16 years (15/17, 94%).
In adults [
n
=
90, age
>
16 years; median 55 (IQR 33–70)],
RHD was the primary cause of HF (
n
=
27; 30%). Hypertensive
cardiomyopathy and presumptive IHD were the most frequent
causes of HFbeyond the sixth decade of life. Overall, hypertensive
cardiomyopathy and IHD ranged as second and third causes of
HF in adults, 24 and 15%, respectively. Other causes are depicted
in Fig. 2C.
Rheumatic heart disease
RHD (
n
=
44) was the main cause of HF in adults and the second
in children. Table 1 shows the echocardiographic features of
RHD. The median age of patients with RHD complicated by
HF was 19 years (12–52) with a
female:maleratio of 2.1:1.
Briefly, the mitral valve was affected in all cases. Mitral
regurgitation was the most common lesion (43/44 cases, 98%)
and the degree of mitral regurgitation was often severe (29/43,
67%). Mitral stenosis was severe in 12 patients (27%). PH (i.e.
pulmonary artery systolic pressures
>
35 mmHg) was present
in 43 subjects [98%; median 65 (50–70 mmHg)]. Moderate and
severe right ventricular dysfunction was present in 27 patients
(61%). Moderate to severe tricuspid regurgitation was present
in 36 patients (82%) due to annular dilatation secondary to RV
remodelling without significant rheumatic involvement.
Representative images of mitral lesions implicated in HF are
shown in Fig. 3. We observed three main patterns of rheumatic
mitral regurgitation: (1) symmetrical restriction of leaflets (30
cases, Fig. 3A); (2) posterior leaflet restriction and anterior
leaflet pseudo-prolapse (eight cases, Fig. 3B); and (3) leaflet
restriction and chordal rupture (five cases; Fig. 3C). Mitral
lesions that did not appear calcified that were deemed suitable
for surgical repair.
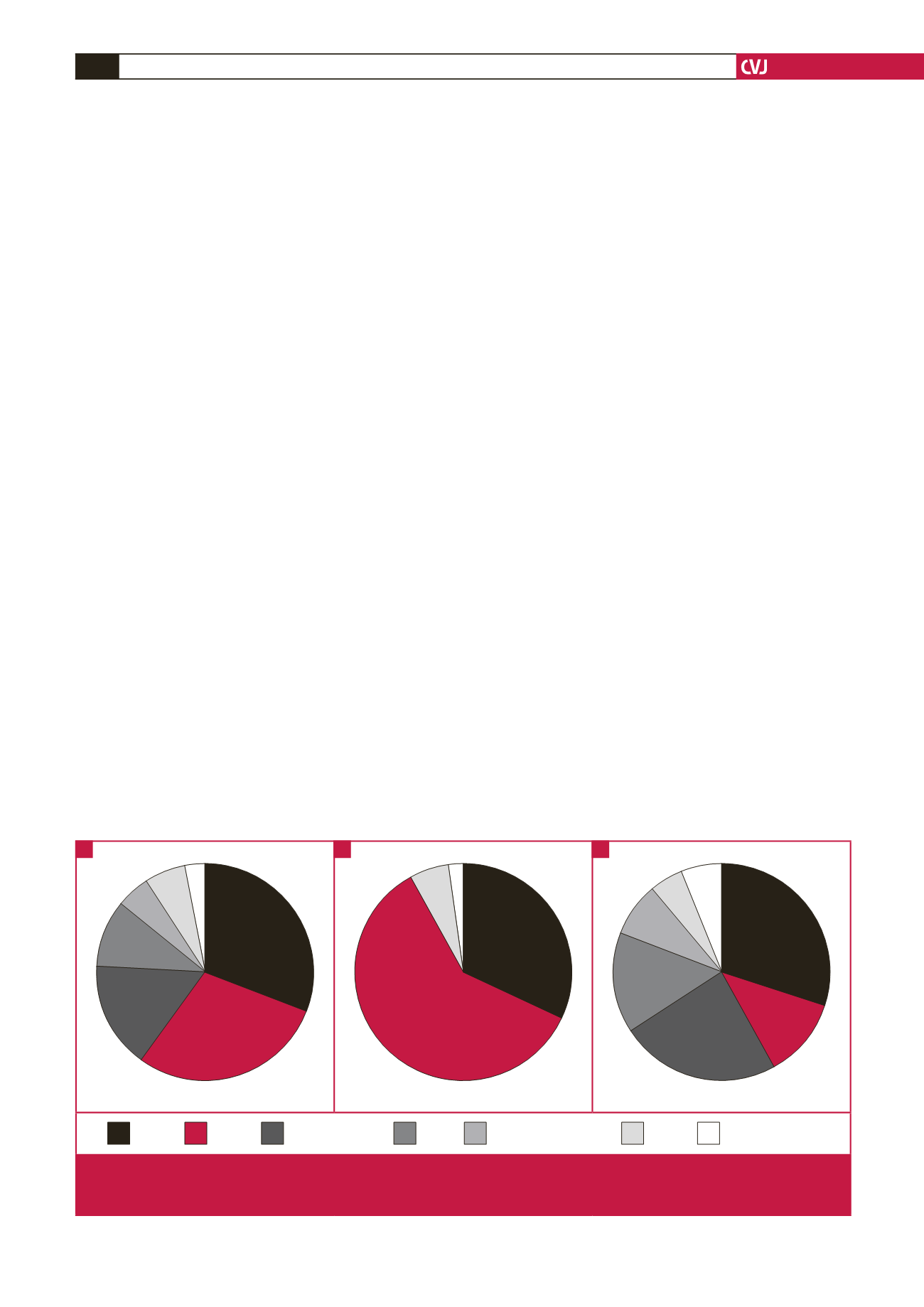
31%
29%
16%
10%
5%
6%
3%
All causes of HF (
n
= 140)
32%
60%
6%
2%
Causes of HF in paediatric subjects (
n
= 50)
30%
12%
24%
15%
8%
5%
6%
Causes of HF in adults (
n
= 90)
RHD
CHD
Hypertension
IHD
RV failure due to
pre-capillary PH
EMF
Other causes
Fig. 2.
Main causes of heart failure (HF) in the study population (A), in paediatric subjects (B), and in adults (C). RHD = rheumatic
heart failure, CHD = congenital heart disease, IHD = ischaemic heart disease, RV = right ventricular, PH = pulmonary
hypertension, EMF = endomyocardial fibrosis.
A
B
C