CARDIOVASCULAR JOURNAL OF AFRICA • Vol 24, No 6, July 2013
210
AFRICA
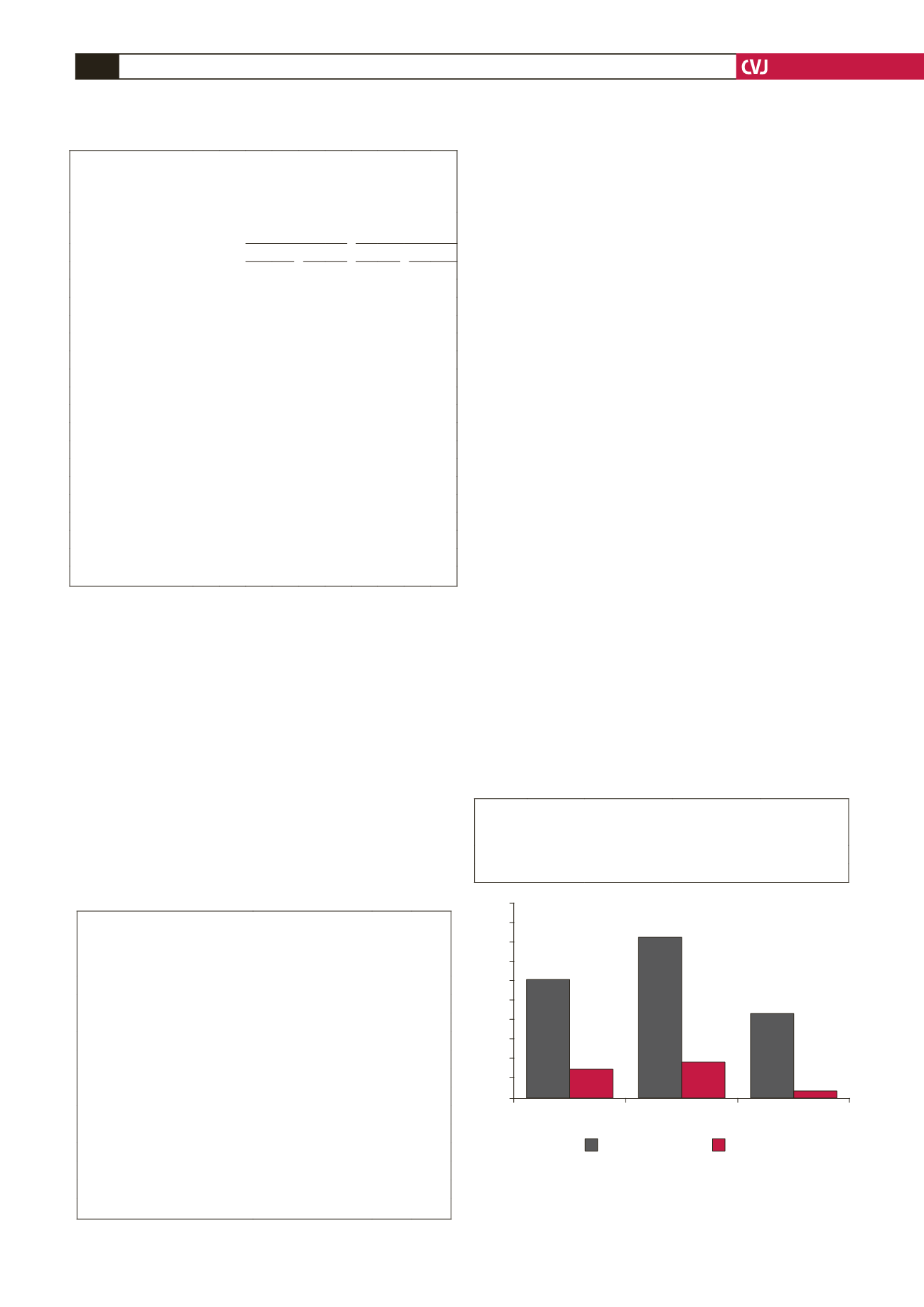
In the whole study group, the number of non-smokers was
104 (52%) compared to 96 (48%) smokers. Of these, smoking
was found in 76 (83%) males and 21 (19%) females (
p
<
0.001).
The number of subjects who were hypertensive and smokers was
40 (43%) males and four (4%) females (
p
<
0.001) (Fig. 1).
BMI estimation showed that 20 (10%) of the study subjects
were of normal weight, 84 (42%) were overweight and 96 (48%)
were obese (Fig. 2). In this study, the relationship of HTN
control with overweight and obesity showed that a higher BMI
had a more detrimental effect on HTN control than a normal
BMI. With regard to BP control, there were 44 (52%) (
p
<
0.03)
subjects in the overweight and 60 (71%) in the obese category
compared to16 (80%) normal-weight subjects. Surprisingly, BP
control in the overweight category was less compared to obese
subjects (Fig. 2).
Discussion
In this study, uncontrolled BP was found in 34% of the subjects,
which is in line with studies in other countries where high levels
of uncontrolled BP were recognised.
13,14
However, the percentages
of uncontrolled BP in this study were higher than that obtained
in other studies.
15,16
This tendency to have uncontrolled BP is
common, even in developed countries such as the USA.
17,18
Our
study suggests a similar prevalence of uncontrolled HTN in
Sudan compared to other countries. However, there has been
a increase in incidence of uncontrolled HTN in Sudan over
the last few years. Further studies are required to determine
suitable methods of BP control to decrease the percentage of
uncontrolled hypertension in the population.
When we considered the risk factors of HTN, this study
revealed that HTN control was better in females than males.
These results are similar to those from previous studies where
females were better protected and achieved better BP control
than males.
19,20
The prevalence of uncontrolled HTN was also
found to be higher in males than females, who were proven to
be protected by the female gender due to the presence of the
hormone oestrogen.
21
Furthermore, male subjects are less likely
to seek medical care.
22
Surprisingly, the level of education showed a positive
association with uncontrolled hypertension in our male subjects,
as the presence of uncontrolled HTN increased with the
educational level. These results are in line with a previous study
done in Sudan.
23
There is no explanation for this association
but we can speculate that HTN in these subjects may have
been complicated by other factors such as stress at work and a
sedentary lifestyle.
Both marital status and employment were found in this study
to be associated with uncontrolled BP in males, although there
was no positive relationship between marriage and lack of
control of HTN in all studies done to date.
24
The negative impact
of marriage on HTN control in our study may have been due
TABLE 2. COMPARISON OF GENDER, MARITAL STATUS,
EDUCATIONAL LEVELAND EMPLOYMENTAND THEIR
RELATIONSHIPWITH LEVEL OF CONTROL OF HTN IN SUBJECTS
WITH CONTROLLED OR UNCONTROLLED HYPERTENSION (
n
=
200)
Blood pressure
Uncontrolled
hypertension
Normal
High
Male Female
Variables
n
%
n
%
n
%
n
%
n
%
Gender
Male
92 46 36 39 56 61 – – – –
Female
108 54 92 85 16 15 – – – –
Marital status
Single
44 22 28 64 16 36 8 50 8 29
Married
148 74 92 62 56 38 48 62 8 11
Widows
4 2 4 100 0 0 0 0 0 0
Divorced
4 2 4 100 0 0 0 0 0 0
Education
Illiterate
32 16 24 75 8 25 8 50 0 0
Primary school
44 22 44 100 0 0 0 0 0 0
Secondary school
80 40 40 50 40 50 32 67 8 53
Higher education
44 22 20 45 25 55 16 67 8 40
Employment
Workers
68 34 40 59 28 41 24 86 4 10
Government-employed 88 44 52 59 36 41 28 50 8 25
Self-employed
44 22 36 82 8 18 4 50 4 11
TABLE 3. DATA REPRESENTINGTHE DESIRE OF PATIENTS TO
CONTRIBUTE TO DECREASINGTHEIR BP BY MONITORING
ITAT HOME,ADHERINGTO DRUG USE, CONTROLVISITS
TOTHE DOCTORAND DIETARY CHANGES (
n
=
200)
Variables
n
%
BP monitoring at home
Yes
40 20
No
160 80
Drug intake as prescribed
Yes
164 82
No
36 18
Efforts to control BP
Yes
172 86
No
28 14
Control visits to doctor
Yes
132 66
No
68 34
Salt in daily meals
Eat with family
104 52
Eat low salt
96 48
Eating salty food (extra salt)
Yes
120 60
No
80 40
Fig. 1. Control of hypertension in smokers and non-
smokers. The table and graph show prevalence of hyper-
tension, and smoking and hypertension in male and
female smokers (
n
=
200).
100
90
80
70
60
50
40
30
20
10
0
Hypertensive
Smoker
Smoker and
hypertensive
%
Males
Females
Number
Hypertension
n
(%)
Smoker
n
(%)
Smoker and
hypertensive
n
(%)
Males
92
56 (61)
76 (83)
40 (43)
Females
108
16 (15)
20 (19)
4 (4)


