CARDIOVASCULAR JOURNAL OF AFRICA • Vol 24, No 6, July 2013
AFRICA
211
to complications from other stresses, risk factors and lifestyle
changes. Low income in Sudan may also be an important stress
factor in marriage. Stress at work could be due to work demands
and low salaries, which would influence the outcome of BP
control.
10,25
The female subjects in all educational groups, marital and
work categories showed better BP control than the males. This
may have been because of the presence of oestrogen, which is
protective against HTN.
21
Moreover females were known to be
better than males in adherence to medication.
26
Other risk factors such as positive family history for HTN
were also evident in this study. This is not surprising as Shehata
et al.
5
found relatives of hypertensive subjects to be more likely
to have HTN early in life.
5
The risk of occurrence of HTN was
found to be greater in subjects with hypertensive first-order
family members.
27
When we evaluated the awareness of HTN and its control, our
data showed a very poor appreciation of HTN and its associated
risks in the study population. The study showed that 54% of our
subjects discovered their HTN when the complications of the
disease became apparent. In the rest of our subjects, HTN was
detected by chance in a routine check-up. These finding suggest
a poor healthcare system and health education programmes.
These results confirm the lack of a national data registry on HTN
in Sudan, which points to a low level of screening and follow
up.
28
Lack of awareness is very significant in the prevalence of
HTN and uncontrolled high BP.
10,16
More attention must be given
to HTN as it is a common risk factor for stroke
29
and kidney
disease,
30
which are recognised to be rapidly increasing in Sudan.
Lack of awareness was evident in our studied subjects.
Compliance with drug usage as prescribed by the doctor was
poor in our study subjects; 18% did not take their medication as
prescribed. In other studies, 11% lack of compliance with drug
use was considered a serious cause of poor treatment of HTN.
31
Some researchers stated compliance with medication to be of
vital importance for good results in the control of HTN.
18,32,33
Lack of awareness in our study subjects can be viewed in
several ways. Only 20% of the study participants went for check-
ups or monitored their BP at home, 14% did not change their
habits to achieve suitable pressure levels and 34% did not visit
doctors on a regular basis. Green
et al
. found that follow up with
doctors and monitoring BP at home resulted in better control.
34
Control of HTN was also influenced by the high sodium intake
found in our study subjects. Increased sodium intake and a
high-salt diet has been proven to be an important aspect in the
prevalence of HTN in the Sudanese population.
35-37
In this study, uncontrolled HTN was found to be prevalent
in smoking males compared to smoking females. In many other
studies, smoking has been recognised as a risk factor for HTN.
38,39
BP levels were found to be higher in hypertensive smokers than
in hypertensive non-smokers.
40
Gender differences with regard
to smoking have not been examined before, but our data are in
line with other studies,
40,41
where smoking was shown to interfere
negatively with the control of HTN.
Overweight and obesity were common among our study
subjects. From this it is evident that overweight and obesity
are among the important risk factors of HTN in the Sudanese
population. Obesity was also noted by Elmahdi
et al
.
42
in a
Sudanese population. A large number of the subjects in our study
who had uncontrolled HTN were overweight or obese. High
BMI is proven to be an important risk factor for HTN.
43,44
Indeed
our finding supports the notion that persistent overweight and
obesity can interfere with the efficacy of hypertension drugs.
45,46
Conclusion
Uncontrolled HTN was associated with lifestyle and risk factors
for HTN and was more prominent in the male gender. The lack of
awareness in the subjects about HTN, its associated risk factors,
changes in lifestyle and adherence to the medication may be a
major factor in the prevalence of uncontrolled HTN in Sudan.
References
1.
Ruilope LM, Schiffrin EL. Blood pressure control and benefits of anti-
hypertensive therapy: does it make a difference which agents we use?
Hypertension
2001;
38
(3 Pt 2): 537–542.
2.
Shapo L, Pomerleau J, McKee M. Epidemiology of hypertension and
associated cardiovascular risk factors in a country in transition: a popu-
lation based survey in Tirana City, Albania.
J Epidemiol Community
Health
2003;
57
(9): 734–739.
3.
Whelton PK, Perneger TV, Brancati FL, Klag MJ. Epidemiology and
prevention of blood pressure-related renal disease.
J Hypertens Suppl
1992;
10
(7): S77–84.
4.
Musaiger AO. Diet and prevention of coronary heart disease in the Arab
Middle East countries.
Med Princ Pract
2002;
11
(Suppl 2): 9–16.
5.
Shehata MF. A proposed study on how far anger contributes to initiat-
ing essential hypertension in Canadian caucasian adults with a family
history of hypertension.
Clin Med Insights Cardiol 2010;
4
: 9–13.
6.
Ghannem H, Fredj AH. Epidemiological transition and cardiovascular
risk factors in Tunisia.
Rev Epidemiol Sante Publique
1997;
45
(4):
286–292.
7.
Tesfaye F, Byass P, Wall S. Population based prevalence of high blood
pressure among adults in Addis Ababa: uncovering a silent epidemic.
BMC Cardiovasc Disord
2009;
9
: 39.
8.
Abu-Aisha H, Elhassan EA, Khamis AH,
et al
.. Rates and causes of
peritonitis in a National multicenter continuous ambulatory peritoneal
dialysis program in Sudan: first-year experience.
Saudi J Kidney Dis
Transpl
2007;
18
(4): 565–570.
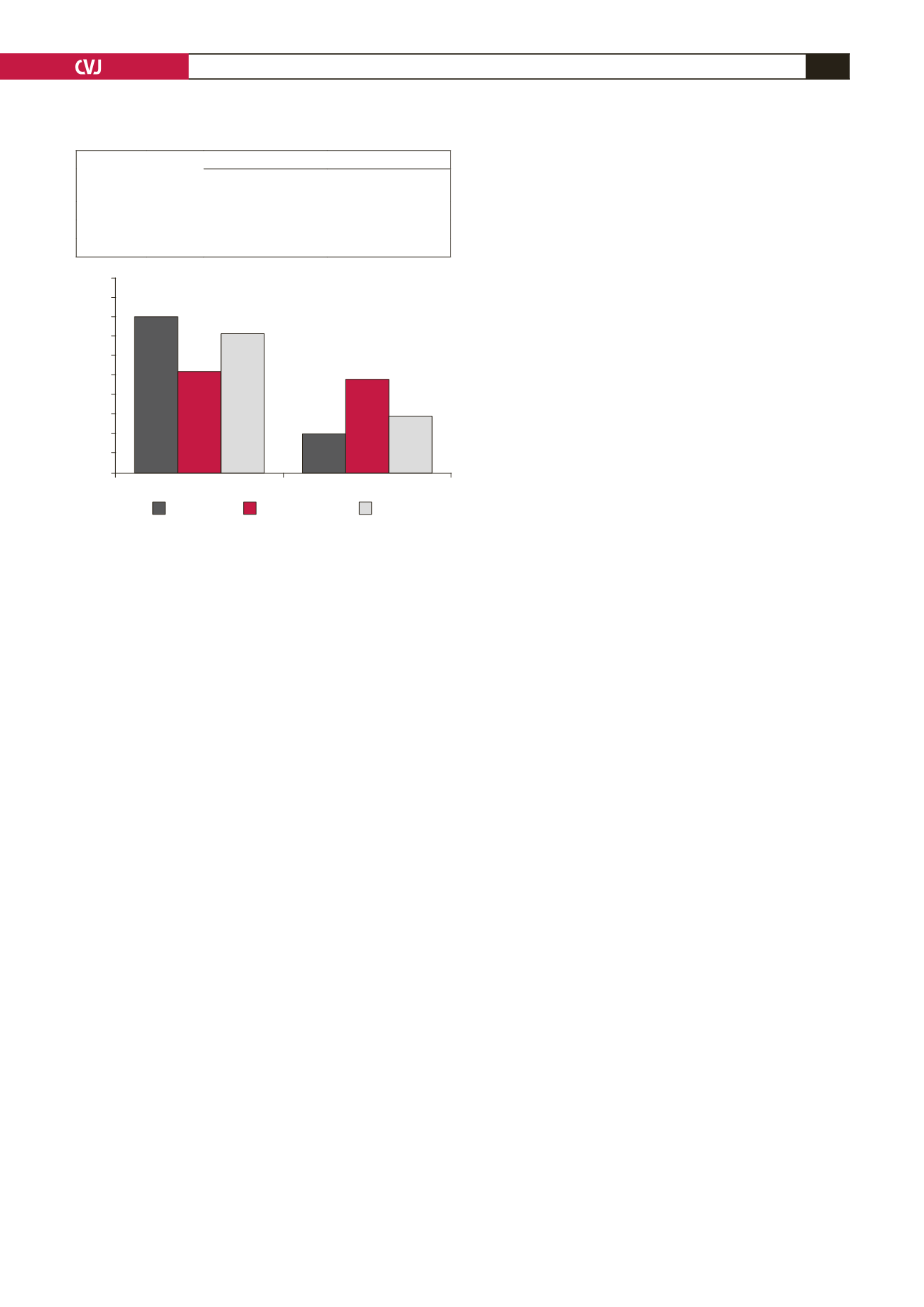
Fig. 2. Effect of overweight and obesity on the control
of hypertension. The table and graph show percentage
of controlled and uncontrolled BP in normal, overweight
and obese subjects (
n
=
200).
100
90
80
70
60
50
40
30
20
10
0
120–160/60–90 mmHg
>140/>90 mmHg
%
Normal
Overweight
Obese
Blood pressure
n
(%)
120–140/60–90 mmHg
n
(%)
>140/>90 mmHg
n
(%)
Normal
20 (10)
16 (80)
4 (20)
Overweight
84 (42)
44 (52)
40 (48)
Obese
96 (48)
68 (71)
28 (29)


