CARDIOVASCULAR JOURNAL OF AFRICA • Vol 24, No 6, July 2013
AFRICA
e5
isolated to the infra-renal aorta with no involvement of the renal
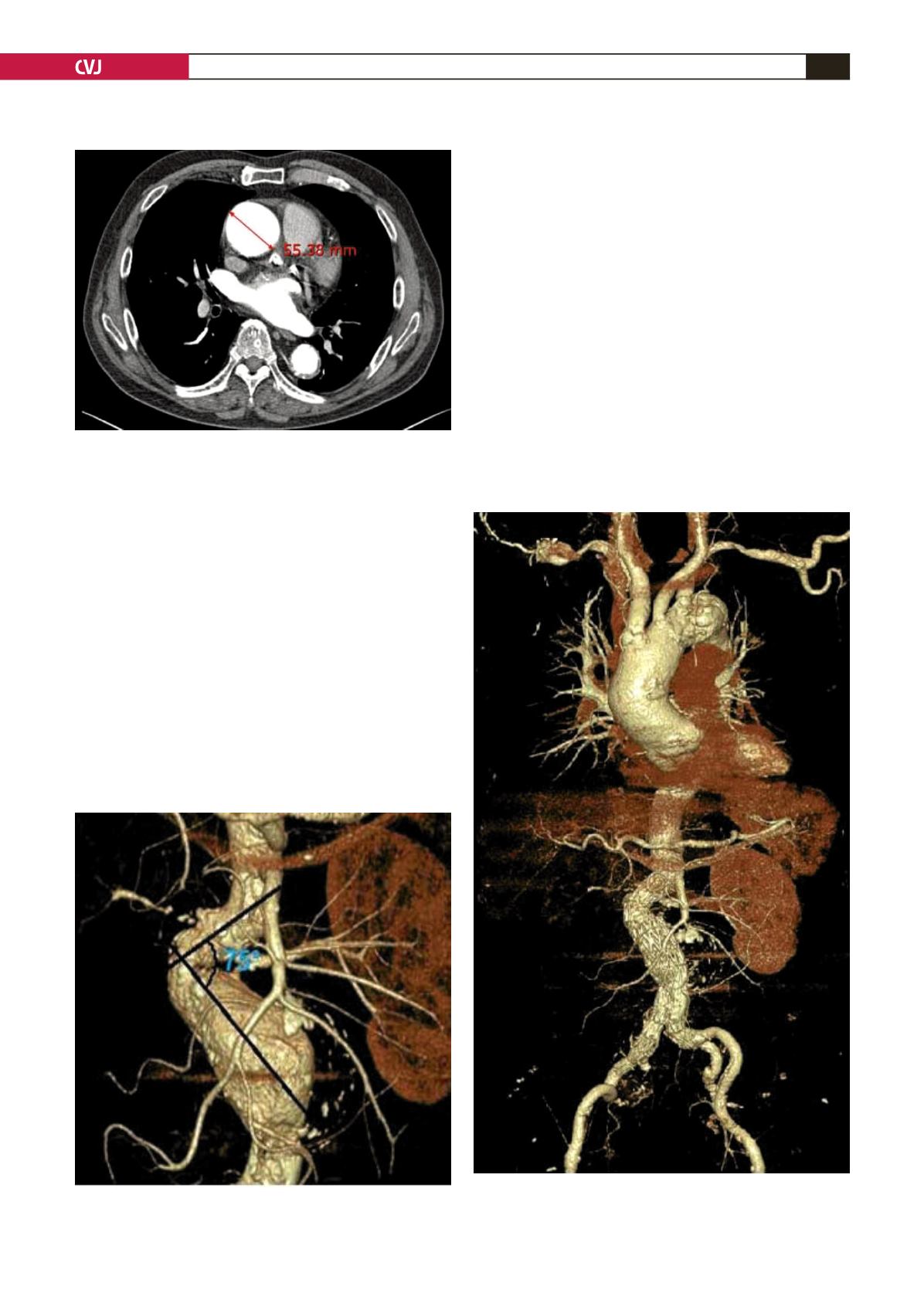
artery. Both iliac arteries and the ascending aorta were dilated
(5.5 cm) (Fig. 2) and it involved the aortic arch.
We discussed with the cardiac surgeon the possibility of
open surgery. He said it did not need elective or emergency
surgery and recommended serial follow up of the change in
the ascending aorta and aortic root diameter. We exclude the
ascending aortic dilation in this report.
After detailed measurements of the length and angle of
the infra-renal neck of the AAA we considered it a debatable
candidate for EVAR due to the short (1.7 cm) and severely
angulated proximal aortic neck (Fig. 3). We had suggested open
surgical repair may be a safer option but the patient had rejected
it. We carefully re-evaluated and measured all aspects of the
aneurysm and the patient’s iliac arteries, as we considered the
patient to be a challenge for stent-graft repair.
He was admitted the afternoon of his procedure. After
lidocaine local anaesthesia, the right common femoral artery
was exposed using a small incision, and the patient underwent
pre-operative, percutaneous plug emobolisation of the outflow
branch of the right internal iliac artery to prevent an endoleak.
Thereafter we deployed a bifurcated stent-graft measuring
28 mm (main body diameter) by 18 mm (iliac limb diameter)
by 11.1 cm (total length) (Zenith
®
, Cook, Inc, Bloomington,
Ind). Through the left femoral artery, a contralateral iliac device
measuring 12 mm (iliac limb diameter) by 7.3 cm (length)
was used. Thereafter an extender cuff was deployed to extend
coverage to the right iliac artery.
The postoperative angiogram showed a proximal type 1
endoleak at the attachment site owing to the severely angulated
proximal neck. We therefore performed several Coda
®
balloon
(Cook, Inc, Bloomington, Ind) dilatations to attach the stent-
graft to its aortic wall. However, the leak remained and we were
undecided between EVAR and open surgical repair.
Fig. 2. The maximum diameter of the aneurismal dilated
ascending aorta was 5.5 cm on CT scan.
Fig. 3. The proximal aortic aneurysmal neck was short
and severely angulated.
Fig. 4. One week later, a follow-up abdominal aorta CT
angiogram showed no visible endoleak and the proximal
aortic neck angle had become more straightened.


