CARDIOVASCULAR JOURNAL OF AFRICA • Vol 24, No 6, July 2013
e6
AFRICA
Unfortunately we were forced to stop the procedure due to the
prolonged procedure time and we did not have a suitable device
at the institution. It was also the start of the Korean New Year
and due to a traffic jam, the delivery of another device would
have been impossible.
The procedure was scheduled for two days ahead. During
those two days we had to find another device, such as an aortic
extender cuff and a Palmaz-Schatz stent
®
(PS 204, Johnson and
Johnson Interventional Systems) to close the endoleak. Palmaz-
Schatz
®
stents were in limited supply in Korea at that time.
We planned two options. First, the use of an aortic extender
cuff was considered. If we failed, a Palmaz-Schatz
®
stent would
be used. Fortunately an aortic extender cuff sized 28 mm (main
body diameter) by 5.8 cm (length) was deployed with success
at the angulated neck. Post-deployment of a Coda
®
balloon
dilatation was also done.
The angle of the proximal aortic neck had also become more
straightened and more closely attached to the aortic wall. We
redid the angiogram and the result was gratifying. The proximal
type 1 endoleak had disappeared so there was no need to use the
Palmaz-Schatz stent
®
.
The patient was discharged on postoperative day 3 with
a normal serum creatinine value. One week later, a follow-
up abdominal aortic CT angiogram was obtained. No visible
endoleak flow was found (Fig. 4). Six months later a follow-up
CT angiogram was done and we could not find any leakage at the
previous graft site. There was however no change in the fusiform
aortic aneurysm in the ascending aorta (Fig. 5).
Discussion
Abdominal aortic aneurysm is a common condition, especially
among older men, and endovascular repair has become a
common treatment option. Numerous reports describe difficulties
in applying EVAR to an aneurysm with ‘hostile neck’ anatomy,
including neck angulation, neck length, associated thrombus and
complex morphology.
4
Sternbergh reported that a patient with severe aortic neck
angulation had a 54 to 70% risk of one or more adverse events.
These outcomes occurred despite adequate length (
>
2 cm) of
the proximal aortic neck. He recommended great caution should
be exercised in recommending EVAR for patients with aortic
neck angulation
≥
40 degrees.
5
In our case the angle of aortic
aneurismal neck was acute (75 degrees) and short (1.7 cm).
ACC/AHA guidelines
6
recommend open or endovascular
repair of infra-renal abdominal aortic anuerysms and/or common
iliac aneurysms is indicated in patients who are good surgical
candidates (Class I, level of evidence A). We agreed that open
surgical repair may have been the more reasonable choice of
treatment. However the patient refused open surgical repair.
After we had obtained informed consent for endovascular repair,
we decided on EVAR.
Conclusion
We obtained a good end result in this case, but we learned much
from it. The surgeon must always ensure there is sufficient
instrumentation to cope with unexpected situations.
References
1.
Parodi JC, Palmaz JC, Barone HD. Transfemoral intraluminal graft
implantation for abdominal aortic aneurysms.
Ann Vasc Surg
1991;
5
:
491–499
.
2.
Greenhalgh R, Brown L, Kwong G, Powell J, Thompson S, EVAR trial
participants. Comparison of endovascular aneurysm repair with open
repair in patients with abdominal aortic aneurysm (EVAR 1), 30-day
operative mortality results: randomized controlled trial,
Lancet
2004;
364
: 843–848.
3.
Mohan IV, Laheij RJ, Harris PL, EUROSTAR collaborators. Risk
factors for endoleak and the evidence for stent-graft oversizing
in patients undergoing endovascular aneurysm repair.
Eur J Vasc
Endovasc Surgery
2001;
21
: 344–349
.
4.
Dillavou ED, Muluk SC, Rhee RY, Tzeng E, Woody JD,
et al
. Dose
hostile neck anatomy preclude successfulendovascular aortic aneurysm
repair?
J Vasc Surg
2003;
38
:
657–663.
5.
Sternbergh WC III, Carter G, York JW, Yoselevitz M, Money SR.
Aortic neck angulation predicts adverse outcome with cardiovascular
abdominal aortic aneurysm repair.
J Vasc Surg
2002;
35
: 482–486.
6.
Rooke T, Hirsch A, Misra S, Sidawy A, Beckman J, Findeiss L,
et
al
. American College of Cardiology Foundation; American Heart
Association Task Force; Society for Cardiovascular Angiography
and interventions; Society of Interventional Radiology; Society for
Vascular Medicine; Society for Vascular Surgery. 2011 ACCF/AHA
focused update of the guideline for the management of patients with
peripheral artery disease (updating the 2005 guideline).
Vasc Med
2011;
16
(6): 452–476.
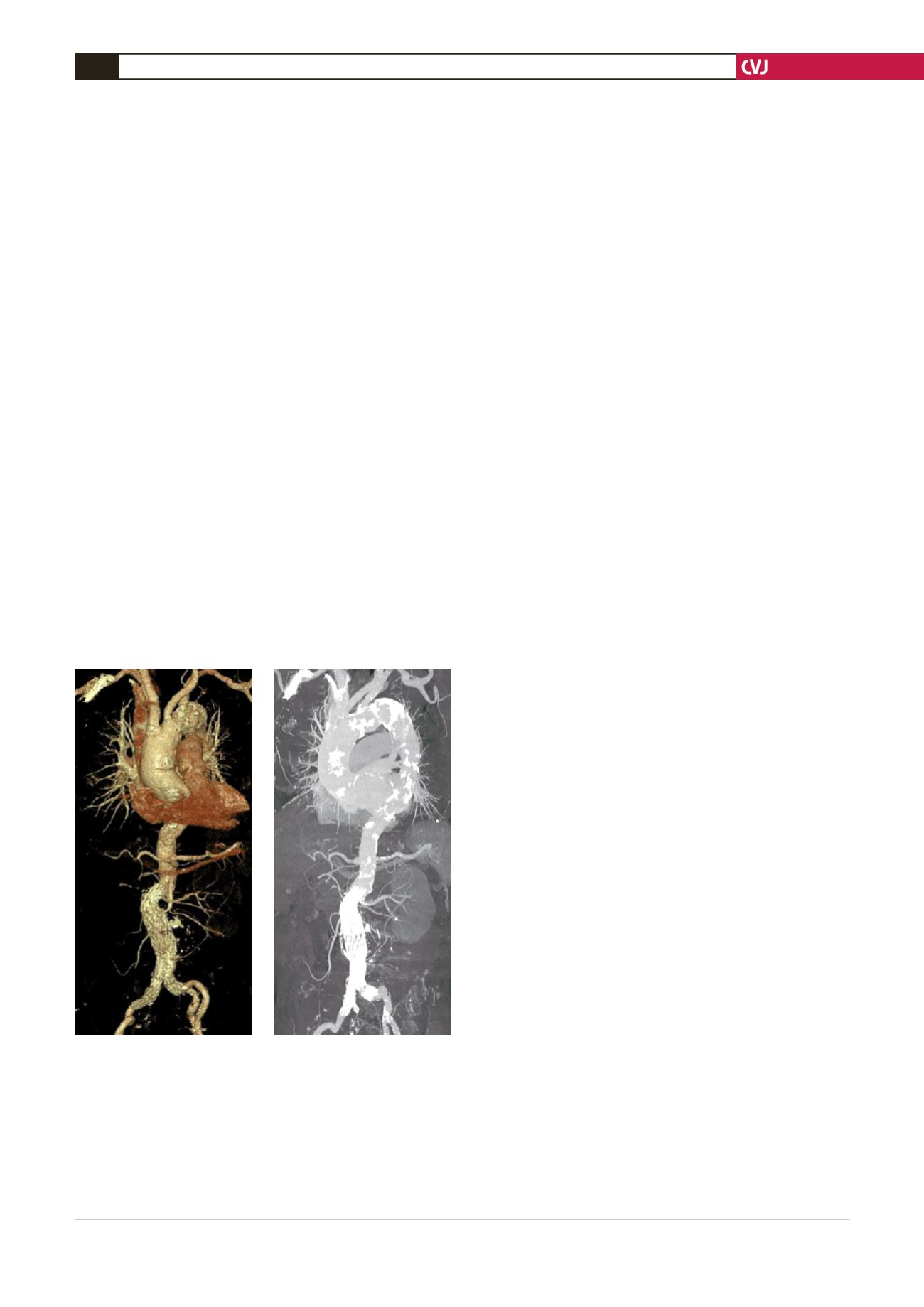
Fig. 5. Six months later, a follow-up abdominal aorta CT
angiogram was done and we could not find any leakage
at the previous graft site. There was also no change in
the fusiform aortic aneurysm size in the ascending aorta.


