
















 22 / 70
22 / 70

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 27, No 5, September/October 2016
292
AFRICA
Discussion
IOBH is a well-known but uncommonly used technique to
remove mass lesions and foreign material such as pacemaker
leads and catheters from the right atrium.
1
In this technique,
blood flow from the superior and inferior vena cavae to the
right atrium is prevented by occlusion with snares, and the
right atrium is then opened. This method has significant
disadvantages, such as bleeding, hypotension, air embolism,
difficulty of surgical exposure, and the necessity to be performed
in a short time. Cardiac and neurological complications may
occur due to systemic and cerebral malperfusion, particularly in
occlusions of more than three minutes.
2
CPB may be required, particularly in cases with complicated
right atrial material. This necessity arises owing to co-morbidities
of the patient, extension of the material, and the potential for
pulmonary embolism. Studies have demonstrated that the use
of CPB is particularly common in cases with co-existence of
extracardiac tumours and large, invasive right atrial thrombus.
4-6
Both IOBH and CPB techniques may be used in the extraction
of intracardiac pacemaker leads,
6
and in tracheal stent
implantation.
7
CPB can alternatively be used for these interventions, but
widespread inflammatory response, length of operation and
intubation times, and duration of intensive care unit and hospital
stays are limitations of the technique.
3
These limitations become
even more apparent in cases with co-morbidities.
1
To overcome
these disadvantages, we have developed a novel double-hole
technique for the removal of foreign material (e.g. catheters,
pacemaker leads) in a bovine heart model.
In the IOBH technique, the superior and inferior vena
cavae should be free from the surrounding tissue. A polyester
tape is placed around each vena cava to provide occlusion of
inflow. Complications such as bleeding and air embolisation
may be minimised in the double-hole technique since it involves
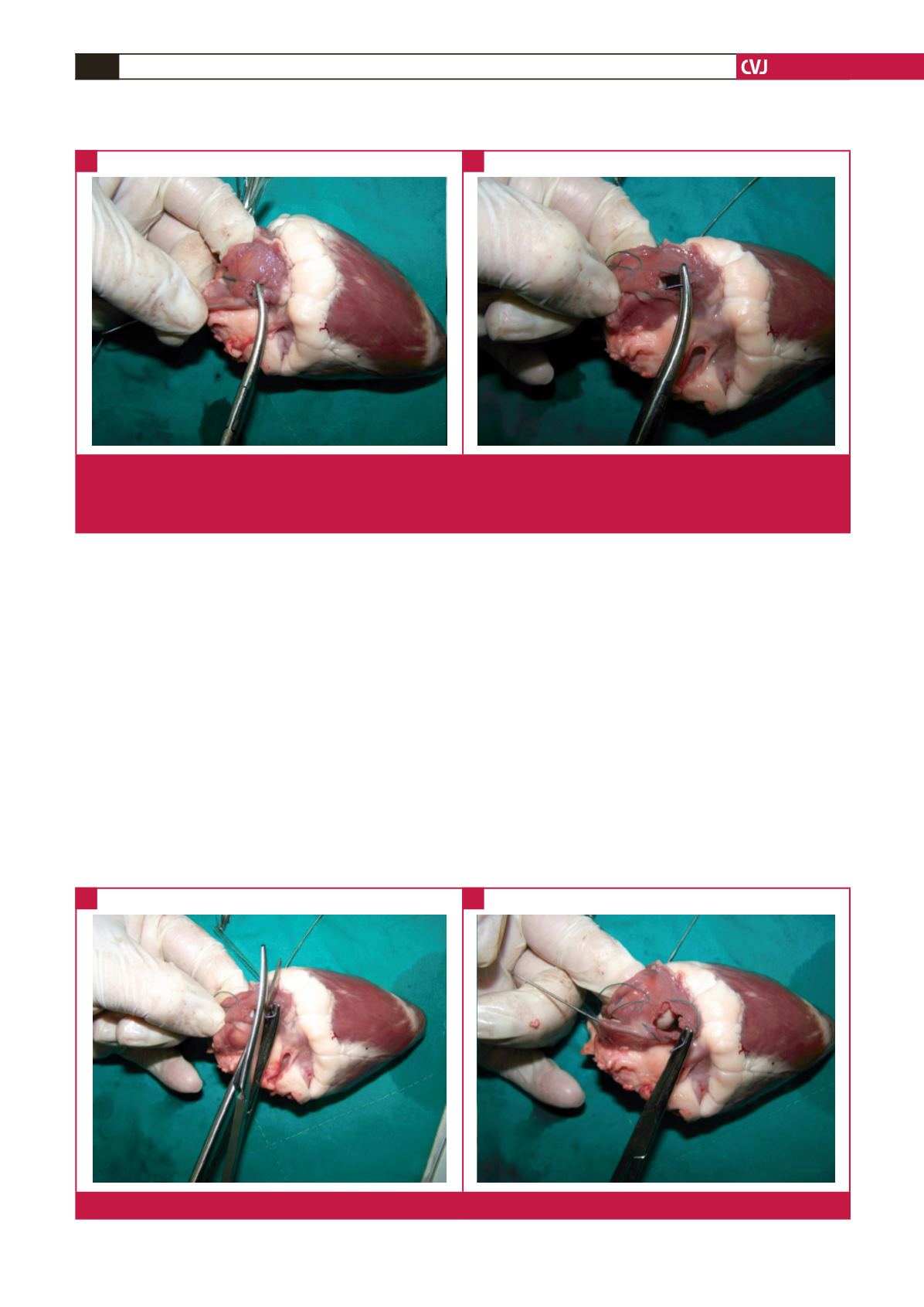
Fig. 1. A.
Two purse-string sutures are placed, one close to the auricle and the other close to the interatrial septum. The left index
finger is inserted into the ventral hole and a closed clamp is inserted into the dorsal hole.
B.
The clamp is opened inside the
right atrium. The clamp is closed after the left index finger pushes the wire between the jaws of the clamp. The wire held by
the clamp is extracted.
A
B
Fig. 2. A.
The extracted wire is cut into two pieces.
B.
Removal of the distal part of the wire.
A
B