
















 55 / 84
55 / 84

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 29, No 2, March/April 2018
AFRICA
117
Diagnostic facilities and challenges
Electrocardiography (ECG):
as shown in Table 2, ECG was
widely available in all African countries, although mainly in
secondary and tertiary health facilities. Signal-averaged ECG
(SA-ECG), which detects arrhythmogenic late potentials for the
diagnosis of arrhythmogenic right ventricular cardiomyopathy/
dysplasia (ARVC/D) was available only in South Africa and in
Maghreb.
Ambulatory ECG monitoring (24-hour Holter-ECG) and
exercise treadmill testing were not routinely performed in many
countries. These tests were available in only 76 and 61% of
the countries, respectively, and they were very expensive. For
instance, in Cameroon, they cost approximately US$180, about
2.7-fold higher than the minimum monthly wage.
Other diagnostic techniques: echocardiography was the most
commonly used imaging technique to rule out or confirm
structural heart diseases. Although widely available in Africa
(Table 2), its use was limited to tertiary centres in larger cities.
Tilt-testing
to rule out vaso-vagal syncope was available in only
six (18.2%) countries (Table 2).
Electrophysiological procedures (EP) for the diagnosis of
paroxysmal advanced heart blocks or tachyarrhythmias were
routinely performed only in countries from North Africa, Kenya,
Senegal and SouthAfrica. Other SSAcountries with implantation
activity were able to supply pacemaker implantations to only
patients with overt conduction system disturbances, excluding
the remaining population with unexplained syncope. A catheter
laboratory was not available in 19 (57.6%) countries (Fig. 1).
Drug challenge aims to unmask silent phenotypes of
inheritable arrhythmogenic diseases such as Brugada syndrome.
However, this test was largely unavailable in many countries of
SSA, with anecdotal reports on ajmaline or flecanide use in some
countries (Fig. 4).
Treatments
Anti-arrhythmia drugs: as shown in the Table 3, digoxin and
amiodarone were the most commonly usedmedications. Vaughan
William’s class I anti-arrhythmic drugs were in short supply,
apart from flecainide, which was present in about 50% of the
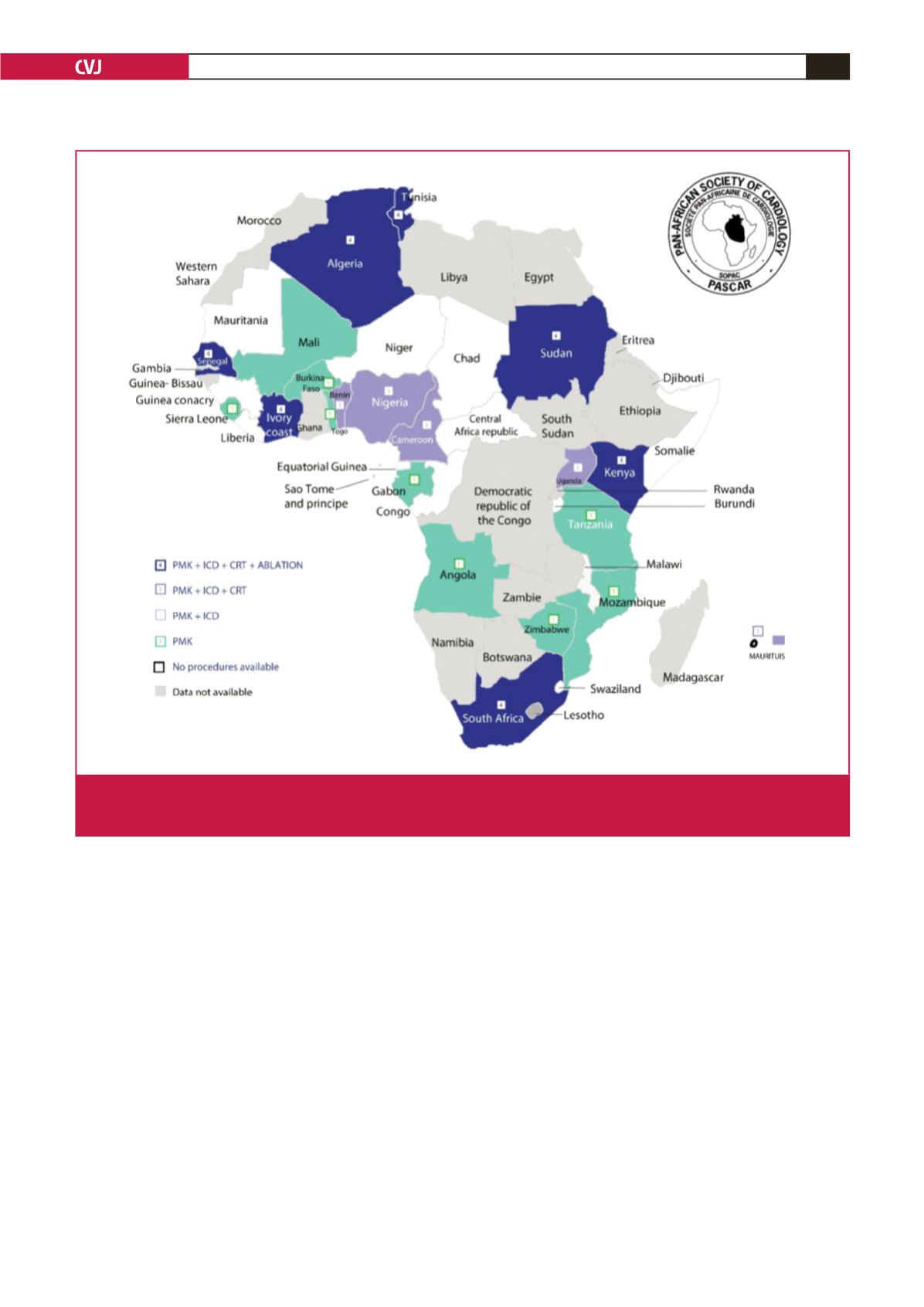
Fig. 1.
Availability of various cardiac arrhythmia services across the African continent. PMK = pacemaker; ICD = implantable cardio-
verter defibrillator; CRT = cardiac resynchronisation therapy. Ablation includes radiofrequency ablation for atrial flutter and
junctional tachycardia (simple ablation) as well as catherter ablation for atrial fibrillation (complex ablation).