
















 49 / 74
49 / 74

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 29, No 5, September/October 2018
AFRICA
311
in echocardiographic parameters and elevated levels of atrial
and B-type natriuretric peptides have been reported in small-
for-date foetuses.
10-13
Our previous study has shown significant
impairment of cardiac function in growth-restricted foetuses,
with the myocardial performance deteriorating with the severity
of growth restriction, as evidenced by increasing MPI values.
5
The MPI was noted to be abnormal before hypoxia or acidosis
set in and can therefore be regarded as a ‘warning’ parameter
of impending compromise. In severe pre-eclampsia it has been
shown that foetal cardiac function was significantly impaired
and deteriorated with worsening degrees of placental vascular
resistance.
6
This project is a continuation of our group’s quest to further
define the clinical use of the MPI in high-risk obstetric conditions
and find its appropriate place in antenatal foetal surveillance, in
the context of present standard foetal-monitoring models. With
this background, the study sought to establish whether a single
elevated MPI value in the third trimester in what can be deemed
stable placental-mediated disease, that is, uncompensated IUGR
or well-controlled pre-eclampsia (single agent and no multi-
systemic manifestation) is a predictor of adverse obstetric
outcome later in the pregnancy.
Methods
Fifty-five foetuses with mothers having stable placental-mediated
disease, either mild pre-eclampsia controlled on a single agent
and/or uncompensated IUGR in the third trimester, attending
the Foetal Unit at Inkosi Albert Luthuli Hospital, Durban,
South Africa were consecutively prospectively recruited. There
were 55 matched controls. This study was approved by the
Biomedical Research Ethics Committee of the University of
Kwa-Zulu Natal, Durban, South Africa (BE228/12).
Uncompensated IUGR was defined as follows: abdominal
circumference
<
10th percentile for gestational age, positive
flow in the umbilical artery but resistance index more than
two standard deviations (2SD) above the mean with no
arterial redistribution, and normal venous Doppler, that is, a
non-hypoxic, non-acidotic growth-restrictive state. Foetuses with
absent or reversed end-diastolic flow in the umbilical artery were
excluded.
Mild pre-eclampsia was defined by the criteria as set out by
the American College of Obstetricians and Gynaecologists
14
as systolic blood pressure
≥
140 mmHg and
<
150 mmHg, or
diastolic blood pressure
≥
90 mmHg and
<
100 mmHg on two
occasions at least six hours apart in a woman on bed rest. This
is accompanied by a proteinuria reading of 1–2
+
on dipstick
testing on two random samples at least six hours apart.
All cases of oliguria (
<
500 ml of urine in 24 hours), cerebral
or visual disturbances, pulmonary oedema, epigastric pain,
impaired liver function and thrombocytopaenia representing
unstable/severe pre-eclampsia at the time of assessment were
excluded. Other exclusion criteria were congenital malformations,
multiple pregnancies, foetuses of diabetic mothers, foetuses
of mothers treated with a tocolytic agent, and foetuses with
abnormal heart rates (tachycardia or bradycardia).
Data recorded for subjects included demographic data of
maternal age and parity, sonographic data of foetal weight
and amniotic fluid index, cardiac Doppler data of MPI, and
foetal Doppler data of umbilical artery (UA), middle cerebral
artery (MCA) and ductus venosus (DV). The cerebro-placental
ratio (CPR) was calculated and plotted on the Ebbing graph to
determine the percentile.
15
Foetal echocardiography using the E8 Voluson General
Electric ultrasound system (GE Medical Systems, WI, USA)
or Siemens Antares ultrasound system (Siemens Medical
Systems, Malvern, PA, USA) was performed in each woman.
The four-chamber view, outflow-tract views, triple-vessel view,
longitudinal view of the aortic and ductal arch, and colour-
flow mapping were used to screen for cardiac malformations.
The MPI was calculated in the foetal left ventricle
4,16
(Fig. 1). Our
previous study established reference intervals and trends of the
MPI in normal pregnancies and the methodology of obtaining the
MPI has been described in detail in the article.
4
A cross-sectional
image of the foetal thorax at the level of the four-chamber view
with an apical projection of the heart was obtained. The Doppler
sample was opened to 3 mm and placed in the internal leaflet
of the mitral valve (MV). In this location, owing to its closeness
to the aortic valve (AV), the opening and closing AV clicks were
registered. The angle of insonation was always
<
30 degrees.
E/A waveform was always displayed as positive flow. The
Doppler gain was lowered as far as possible to clearly visualise
the echoes corresponding to the opening and closing clicks of
the two valves at the beginning and end of the E/A (mitral valve)
and aortic waveforms. Cruz-Martinez
et al.
17
suggested using the
beginning of the mitral and aortic valve clicks as the landmarks
for measurement but this can lead to poorer variability and
varying results due to variation in valve click widths.
Measurement of the time intervals at the peak of the valve
clicks was used as it overcomes this problem, and is more
precisely definable than the base, as was performed in our
normal reference values study, showing excellent reproducibility,
4
and also as suggested by Meriki
et al
.
18
This is a clearer landmark
and overcomes variations in valve click width and has a better
reproducibility.
The Doppler sweep velocity was set at 5 cm/s and the wall
motion filter at 300 Hz. The three time periods were estimated
as follows: ICT – from the beginning of the MV closure to the
AV opening; ET – from the AV opening to closure; IRT – from
AV closure to MV opening. The modified MPI (Mod-MPI)
=
(ICT
+
IRT)/ET. The peak of the click was used as the
landmark, as suggested by Meriki
et al
.,
18
as this results in better
reproducibility.
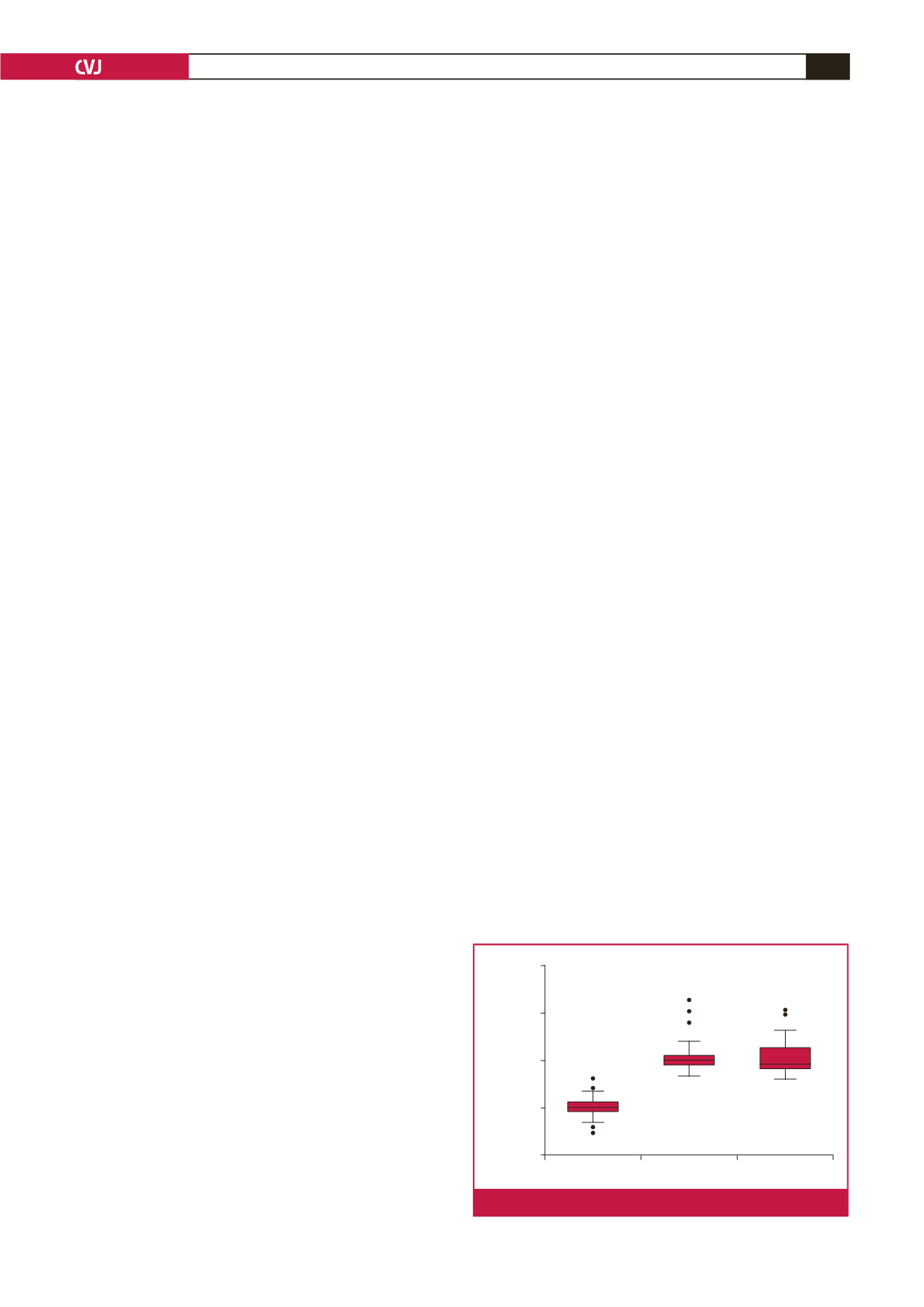
Control
IUGR
PE all
MPI
z
-score
15
10
5
0
–5
Fig. 1.
MPI
z
-score versus controls, IUGR and PE group.