


















 57 / 64
57 / 64

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 31, No 3, May/June 2020
AFRICA
e1
Early Supera stent fracture in the femoropopliteal artery
Hun-Tae Kim, Jeong-Hwan Cho, Jung-Hee Lee, Ung Kim
Abstract
The Supera peripheral stent has been designed to resist stent
fracture, which can develop from the torsion and compres-
sive forces in the femoropopliteal artery. We report on a case
of Supera peripheral stent fracture in the early period after
the index procedure in a patient with femoropopliteal artery
disease. An individualised approach, considering the lesion
location, patient’s age and exercise capacity is important for
the treatment of femoropopliteal artery disease.
Keywords:
peripheral artery disease, popliteal artery occlusion,
Supera interwoven nitinol stent, stent fracture
Submitted 13/10/19, accepted 29/1/20
Published online 17/3/20
Cardiovasc J Afr
2020;
31
: e1–e3
www.cvja.co.zaDOI: 10.5830/CVJA-2020-004
The Supera peripheral artery stent (Abbott, CA, USA) has an
interwoven nitinol design that allows it to mimic the natural
movement of the anatomy and supports the vessel with minimal
chronic outward force. Therefore, Supera stents can be effective
when treating the dynamic environment of the superficial femoral
artery and proximal popliteal artery. While observational data
has supported its use, some complications have been reported.
1-3
Here we present a case with a Supera peripheral stent fracture 12
days after stent implantation in the femoropopliteal artery.
Case report
A 73-year-old male patient visited our hospital complaining of
right leg claudication (Fontaine stage IIb, Rutherford category
3) over three months. His past medical history and laboratory
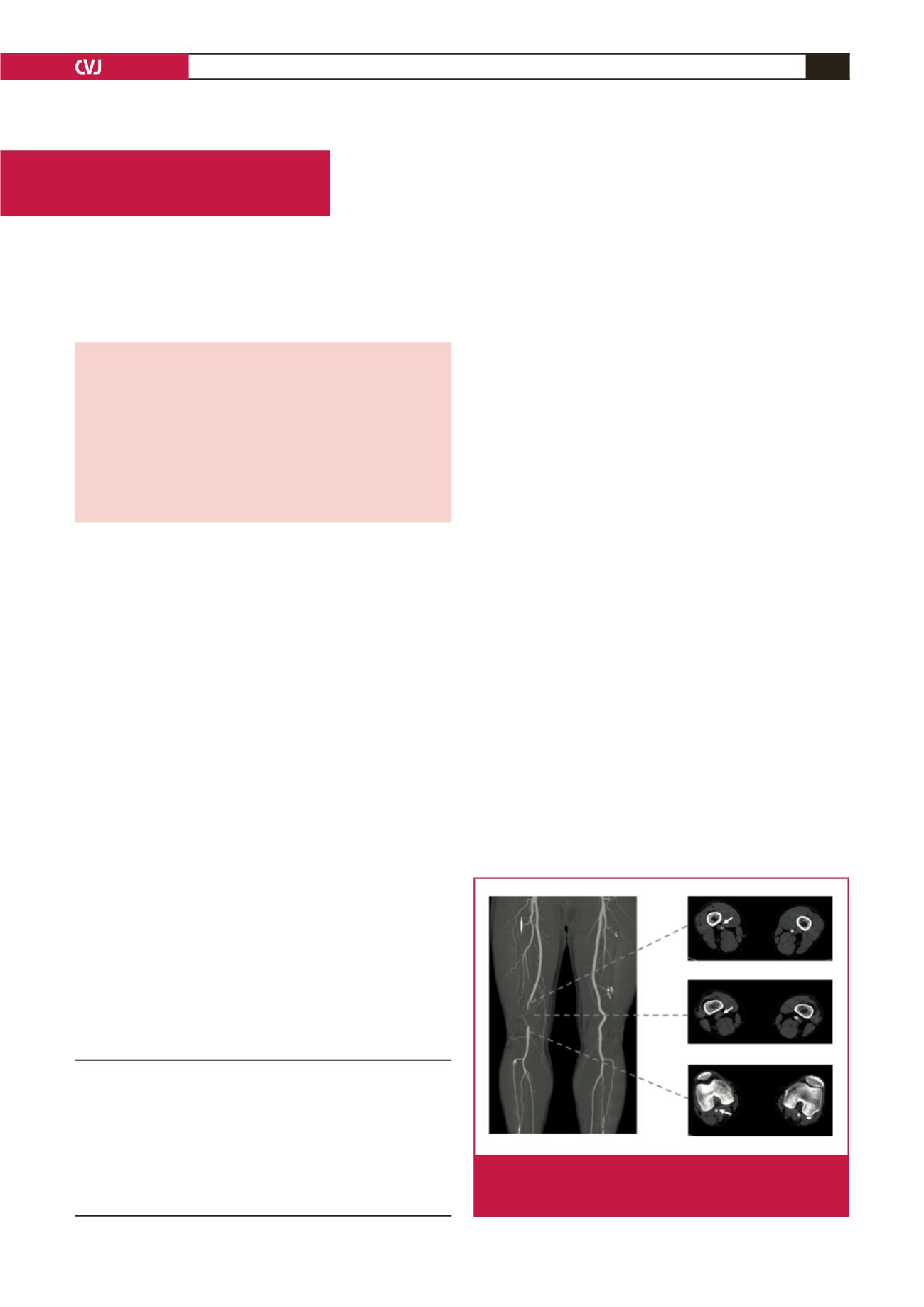
results were non-specific. Non-invasive studies of ankle–
brachial index (ABI) and lower extremity computed tomography
(CT) angiography showed right femoropopliteral artery total
occlusion (Fig. 1).
The patient underwent percutaneous transluminal
angiography (PTA) through the ipsilateral femoral artery (6
French, Ansel
®
sheath, Cook Medical, IN, USA) (Fig. 2A)
using microcatheter support (CXI
®
, Cook Medical, IN, USA).
A 0.014 wire (Command ES
®
, Abbott, CA, USA) was used for
lesion crossing. As required by the Supera stent instructions
for use,
3
sequential predilatation of the femoropopliteal lesion
was performed (Admiral Xtreme
®
5 × 80 mm, Medtronic, MN,
USA) and the Supera 5 × 80-mm stent was implanted. A final
angiogram showed good patency of the right popliteal artery
with no residual disease (Fig. 2B) and post-PTA ABI was 1.07.
However, 12 days later, he visited our hospital and complained
of claudication again. ABI was 0.62 and lower extremity CT
angiography showed stent fracture with right popliteal artery
total occlusion (Fig. 3A). We performed secondary PTA. The
angiogram showed stent fracture (type V),
4
with a large amount
of thrombus in the area of the Supera stent (Fig. 3B, C).
Thrombus aspiration was done and a 0.035 wire (Terumo
®
,
TerumoMedical Corporation, Tokyo, Japan) was passed through
the back-up of the guiding catheter (Glide
®
, Terumo Medical
Corporation, Tokyo, Japan). After popliteal filter deployment,
balloon angioplasty (Admiral Xtreme
®
5 × 60 mm, Medtronic,
MN, USA) was performed and drug-coated balloon angioplasty
(Lutonix
®
5 × 120 mm, Bard, AZ, USA) was applied. The final
angiogram showed good patency of the stent (Fig. 3D) and post-
PTA ABI was 0.9.
Unfortunately, claudication developed again three days after
repeated PTA. We transferred the patient to the vascular surgeons
and bypass surgery between the superficial femoral artery and
Divison of Cardiology, Yeungnam University Medical
Centre, Daegu, Republic of Korea
Hun-Tae Kim, MD,
hto423@hanmail.netJung-Hee Lee, MD, PhD
Ung Kim, MD, PhD,
woongwa@yu.ac.krDivision of Cardiology, Daegu Veterans Hospital, Daegu,
Republic of Korea
Jeong-Hwan Cho, MD
Case Report
Fig. 1.
Lower extremity with computed tomography. White
arrows indicate the right femoropopliteal artery with
total occlusion in the P2 segment.