CARDIOVASCULAR JOURNAL OF AFRICA • Vol 21, No 1, January/February 2010
AFRICA
53
Drug Trends in Cardiology
Treating hypertensive patients with coronary artery disease:
renewed interest in INVEST
The INVEST study, a very large study of
22 576 hypertensive patients with coro-
nary artery disease (CAD)
1
has recently
been reviewed in the context of more
recent studies, such as ASCOT
2
and
ACCOMPLISH,
3
all of which focused on
the use of a calcium channel blocker-led
(CBB) strategy in combination with an
ACE inhibitor to reduce cardiovascular
events.
The Cardiovascular Journal of
South Africa
, precursor to the present
Cardiovascular Journal of Africa
,
published expert comment on the results
of the INVEST trial in 2003 and reported
on the follow-up series of meetings held
in South Africa after the 2003 American
College of Cardiology (ACC) meeting
at which the INVEST trial results were
presented.
4
Particularly important for our
diverse society is that this trial included
13% black patients, and 52% of the
patients were female.
Essential to the understanding of the
INVEST study is the context in which it
was initiated in the mid-nineties; main-
ly to address unanswered management
issues in patients with CAD. At that
time, diuretics and
β
-blockers were the
standard blood pressure-lowering therapy,
although they had not been shown to
reduce morbidity and mortality to the
levels predicted from epidemiological
studies. The newer agents such as CCBs
and ACE inhibitors were increasingly
being used, although outcome data were
lacking at the time.
The INVEST study focused on hyper-
tensive patients with CAD who were older
than 50 years. It anticipated that very few
patients would achieve target blood pres-
sure on monotherapy and opted to test the
combined use of verapamil SR 240 mg/
day and trandolapril 4 mg/day against
atenolol (twice daily) and hydrochloro-
thiazide (HCTZ) (Fig. 1). Patients were
monitored every six weeks for the first six
months, and then every six months until
the study end (mean follow-up period 2.9
years).
The overall objective of INVEST
was to compare the risk for the primary
outcome (PO), defined as all-cause death,
non-fatal myocardial infarction (MI) or
non-fatal stroke, following treatment with
the two strategies. Secondary outcomes
included not only all-cause death, non-
fatal MI and non-fatal stroke individually,
but also new-onset diabetes and trends
for cancer, Parkinson’s, Alzheimer’s and
autoimmune disease and gastrointestinal
bleeding, since these had all been anec-
dotally attributed to long-term use of
calcium antagonists.
Depression is common in CAD
patients and is an important risk factor for
subsequent coronary heart disease (CHD)
events.
5
Because the use of
β
-blockers
may be associated with generalised
fatigue and depression, the substudy
Antihypertensive Drugs and Depression
Symptoms (SADD-Sx)
6
was carried out
to examine the tolerability of the two
strategies and to assess for depression at
baseline and after one year of treatment.
For the substudy, 2 317 consecutively
randomised INVEST patients in the USA
were mailed questionnaires, including a
sociodemographic survey at baseline and
the Centre for Epidemiologic Studies –
Depression (CES-D) scale at baseline and
after one year of study participation.
Another ongoing substudy included
ambulatory blood pressure monitor-
ing (ABPM), in which a portion of the
INVEST population underwent ABPM at
baseline and after one year of follow up.
TABLE 1. KEY FINDINGS OF INVEST
A verapamil SR-plus-trandolapril strat-
●●
egy was equivalent to an atenolol (twice
daily)-plus-hydrochlorothiazide strategy
with regard to reduction in cardiovascular
outcomes, with similar blood pressure
reduction and control
The verapamil SR plus trandolapril strat-
●●
egy was associated with a reduced risk
for new-onset diabetes
Elderly patients with hypertension and
●●
CAD require multi-drug therapy for
blood pressure control. Lean, elderly
patients should be treated carefully and
blood pressure should not be lowered too
far in this population
Blood pressure reduction and reduction
●●
in angina episodes were associated with
an improved feeling of well being
Atenolol, when dosed twice daily, was
●●
not associated with increased risk of
stroke or other adverse cardiovascular
outcomes
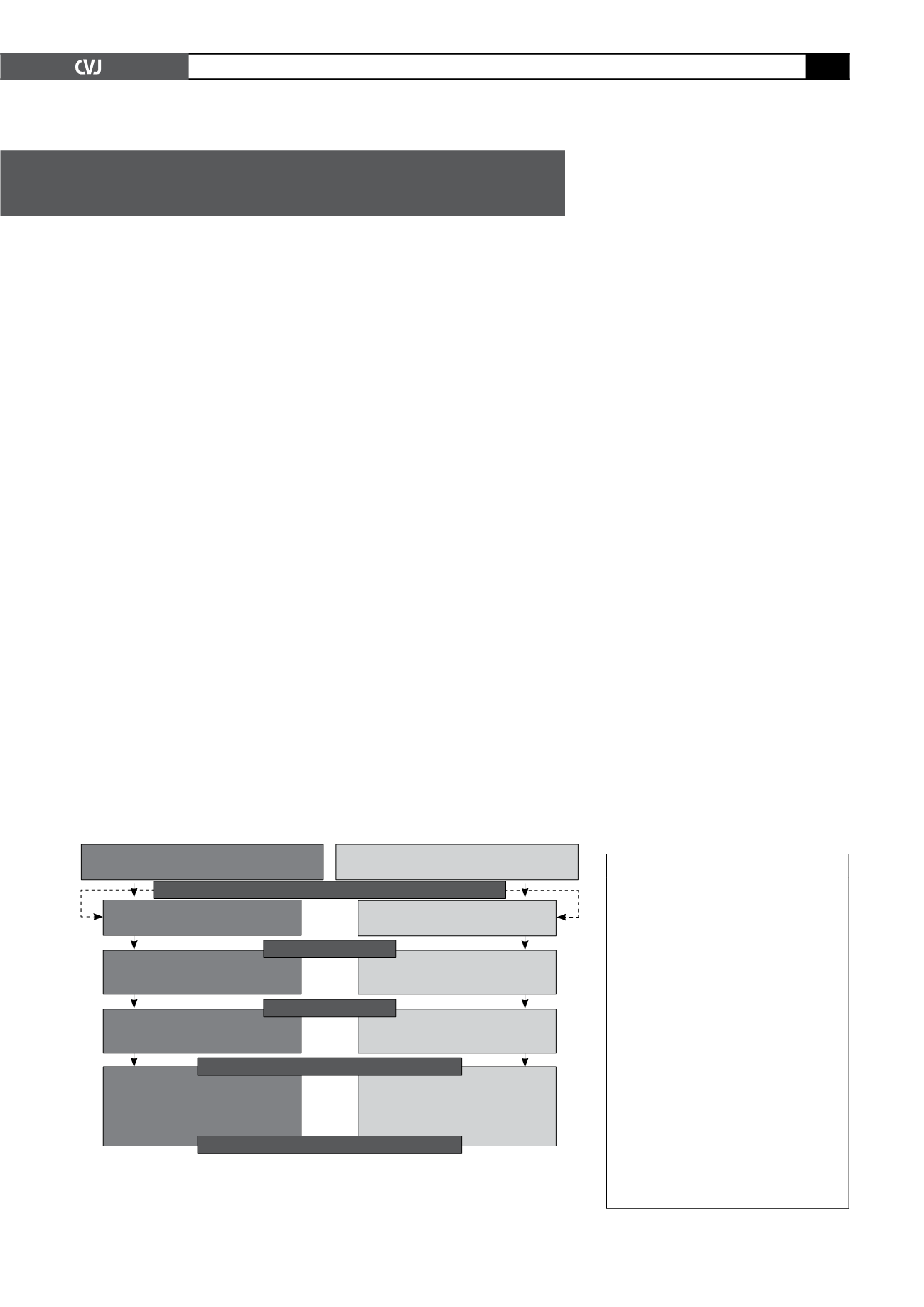
Fig. 1. INVEST treatment strategies. The drugs, order of addition and recom-
mended doses for each step of each strategy are summarised. Non-study
antihypertensive drugs could be added to control blood pressure except for
β
-blockers in those assigned to the atenolol arm.
Verapamil SR Strategy
Atenolol Strategy
Step 1
Verapamil SR 240mg
Step 1
Atenolol 50mg
Step 2
Verapamil SR 240mg
+ Trandolapril 2mg
Step 2
Atenolol 50mg
+ HCTZ 25mg
Step 3
Verapamil SR 180mg twice daily
+ Trandolapril 2mg twice daily
Step 3
Atenolol 50mg twice daily
+ HCTZ 25mg twice daily
Step 4
Verapamil SR 180mg twice daily
+ Trandolapril 2mg twice daily
+ HCTZ 25mg
Step 4
Atenolol 50mg twice daily
+ HCTZ 25mg twice daily
+ Trandolapril 2mg
Diabetes, Renal Dysfunction, Heart Failure – Add Trandolapril
Addition of Drug
Increase Dose
Addition of Drug or Add Nonstudy Drug
Increase Dose and/or Add Nonstudy Drug(s)


