CARDIOVASCULAR JOURNAL OF AFRICA • Vol 21, No 1, January/February 2010
48
AFRICA
from malignancies or hepatic disease.
3
Prevalence is estimated at
between 0.5 and 2.6%, but this is influenced by the methodology
used and the population selected.
3
The exact mechanism resulting in CK molecules forming
complexes with immunoglobulins remains largely unknown.
Due to the high molecular weight of macro-CK, renal clearance
is reduced, resulting in an increased half life of the complex.
4
CK
does not have an extracellular catalytic function; so although of
no pathological consequence to the patient, the macro-molecule
retains enzymatic activity analytically and interferes with total
CK and CKMB activity assays, leading to false positive results.
2
CK catalyzes the reversible phosphorylation of creatine and
adenosine triphosphate (ATP) to form creatine phosphate and
adenosine diphosphate (ADP). In the routine laboratory, total
CK activity is commonly determined by measuring either the
forward or reverse products of the reaction.
5
Several methods are
available for the measurement of the CKMB isoenzyme.
In the CKMB immuno-inhibition activity assay, an anti-
body is used to inhibit the CKM moiety of the CKMB and the
CKMM. The resultant CKBB and CKB moiety of the CKMB
is then measured similarly to the total CK activity mentioned
previously. This method is based on the premise that normally
insignificant amounts of CKBB are present in the serum and
therefore the CKB moieties measured reflect the amount of
CKMB activity in the specimen. It is understandable then that
the presence of macro-CK (most commonly a CKBB complex)
will falsely elevate the CKMB activity result.
CKMB can also be measured by mass assay. The most
common approach to measuring mass is with an immunometric
method using antibodies directed against the M or B subunit.
Because of the CKMB specificity of the antibodies used, inter-
ference poses less of a problem.
5
A disadvantage is that the mass
assay is much more expensive.
An alternative approach to excluding macro-CK interfer-
ence in a CKMB activity assay would be to have the specimen
re-analysed, if available, with a mass assay. When macro-CK
interference is suspected in a total CK assay, as requested for
the diagnostic workup of muscle disorders or drug side effects,
routine method alternatives are unfortunately not available.
Screening by PEG precipitation or analysis by CK electrophore-
sis or gel filtration chromatography remains the only option.
These methods are available only in specialised laboratories.
Although cardiac troponin has become the preferred biomark-
er for cardiac damage, the 2007 American College of Cardiology
and American Heart Association guidelines for the management
of patients with unstable angina/non-ST-elevation myocardial
infarction state that the determination of CKMB remains useful
for the diagnosis of early infarct extension and periprocedural
infarction.
6
Although CKMB mass assays are recommended, guide-
lines published in 2007 by the National Academy of Clinical
Biochemistry and the International Federation of Clinical
Chemistry state that CKMB activity assays are still an accept-
able alternative to mass assays in institutions where mass assays
are not available or feasible.
7
Analytically, troponin immunoassays are also not without
problems. False positive results due to macro-troponin, as well
as false negative results due to anti-troponin antibodies have
been described.
4
Conclusion
Although well described, analytical interference due to macro-
complexes remains an underestimated and unrecognised prob-
lem. In our experience, clinical awareness is not optimal. Not
recognising these interferences can lead to misdiagnosis and
mismanagement of patients.
The patient’s chest pain resolved spontaneously and she was
discharged. On follow up, the patient has been well, despite the
biochemical pattern remaining unchanged.
This case illustrates the importance of good communication
between the clinician and the pathologist in optimising patient
care.
References
Fahie-Wilson MN, Burrows S, Lawson GJ, Gordon T, WongW, Dasgupta
1.
B. Prevalence of increased serum creatine kinase activity due to macro-
creatine kinase and the experience of screening programmes in district
general hospitals.
Ann Clin Biochem
2007;
44
: 377–383.
Rameley AT, Wilding P. Macroenzymes: biochemical characterization,
2.
clinical significance and laboratory detection.
Clin Chem
1989;
35
:
2261–2270.
Panteghini M, Bais R, van Solinge WW. Enzymes. In: Burtis CA,
3.
Ashwood ER, Bruns DE, eds. Tietz
Textbook of Clinical Chemistry and
Molecular Diagnostics
, 4th edn. Elsevier Saunders, 2006:
599
.
Wu AHB. Cardiac troponin: friend of the cardiac physician, foe to the
4.
cardiac patient?
Circulation
2006;
114
: 1673–1675.
CD ROM: CK methods. In: Kaplan LA, Pesce AJ, Kazmierczak SC, eds.
5.
Clinical Chemistry Theory, Analysis, Correlation
, 4th edn. Mosby, 2003.
ACC/AHA 2007 Guidelines for the management of patients with unsta-
6.
ble angina/non-ST-elevation myocardial infarction – executive summary.
J Am Coll Cardiol
2007;
50
: 652–726.
National Academy of Clinical Biochemistry and IFCC committee
7.
for standardization of markers of cardiac damage laboratory medi-
cine practice guidelines: analytical issues for biochemical markers of
acute coronary syndromes.
Circulation
2007 [cited 2008 Sep 9]; 115;
e352-355. Available from:
/
full/115/13/e352.
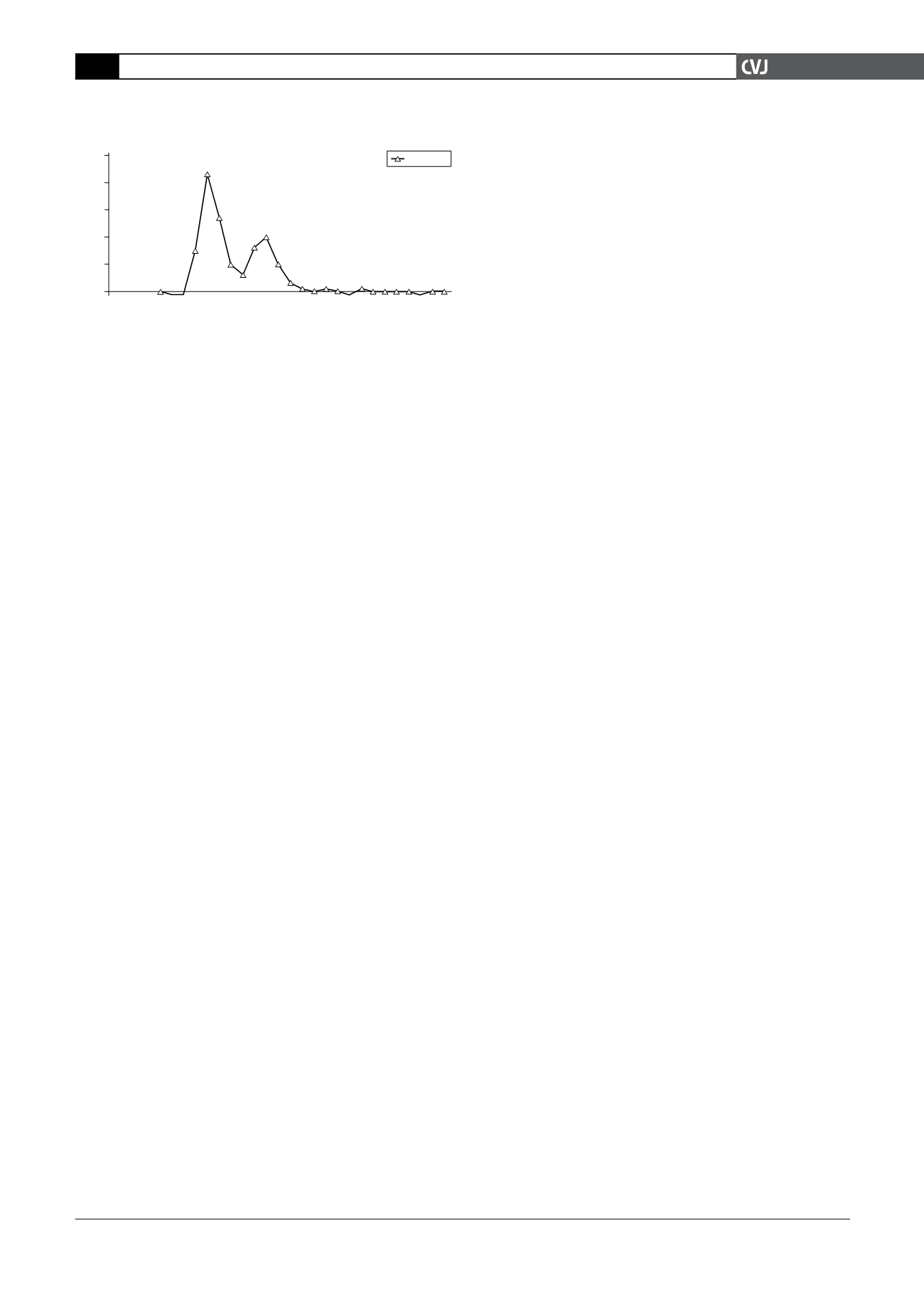
Fig. 1. Gel filtration chromatography demonstrating the
presence of predominantly macro-CK in the patient
specimen. Note that the free CK is well within the normal
population reference range.
50
40
30
20
10
0
CK IU/l
35
45
55
65
75
Macro-CK
Free CK
Eleunt volume (ml)
CK IU/l


