CARDIOVASCULAR JOURNAL OF AFRICA • Vol 23, No 1, February 2012
AFRICA
e19
2 5 S ptember/October 2011
275
TEE was performed in both patients six months after placement
and showed good positioning of the devices and no residual
shunting.
Discussion
PFO closure in patients with ischaemic stroke and those with
migraine remains controversial.
13-15
This can be attributed to the
fact that most studies of device closure for these patients are
observational in nature, as well as the overall lack of randomised
controlled clinical trials. As a direct result, no clear guidelines
for closure exist. The American Heart Association, American
Stroke Association and the American College of Cardiology
Foundation therefore, in a statement, called on physicians to
consider participation in currently ongoing prospective trials in
order to resolve these issues.
16
This is the first reported use of the Cardia
©
PFO device in
South Africa. The Atriasept™ II PFO occluder is a self-expand-
able, double-disc device with a skeleton of nitinol wires, each
covered with a polyvinyl-alcohol membrane and is available in
sizes of 20, 25, 30 and 35 mm. The two discs are linked by a
self-centring mechanism, which allows some angulation of each
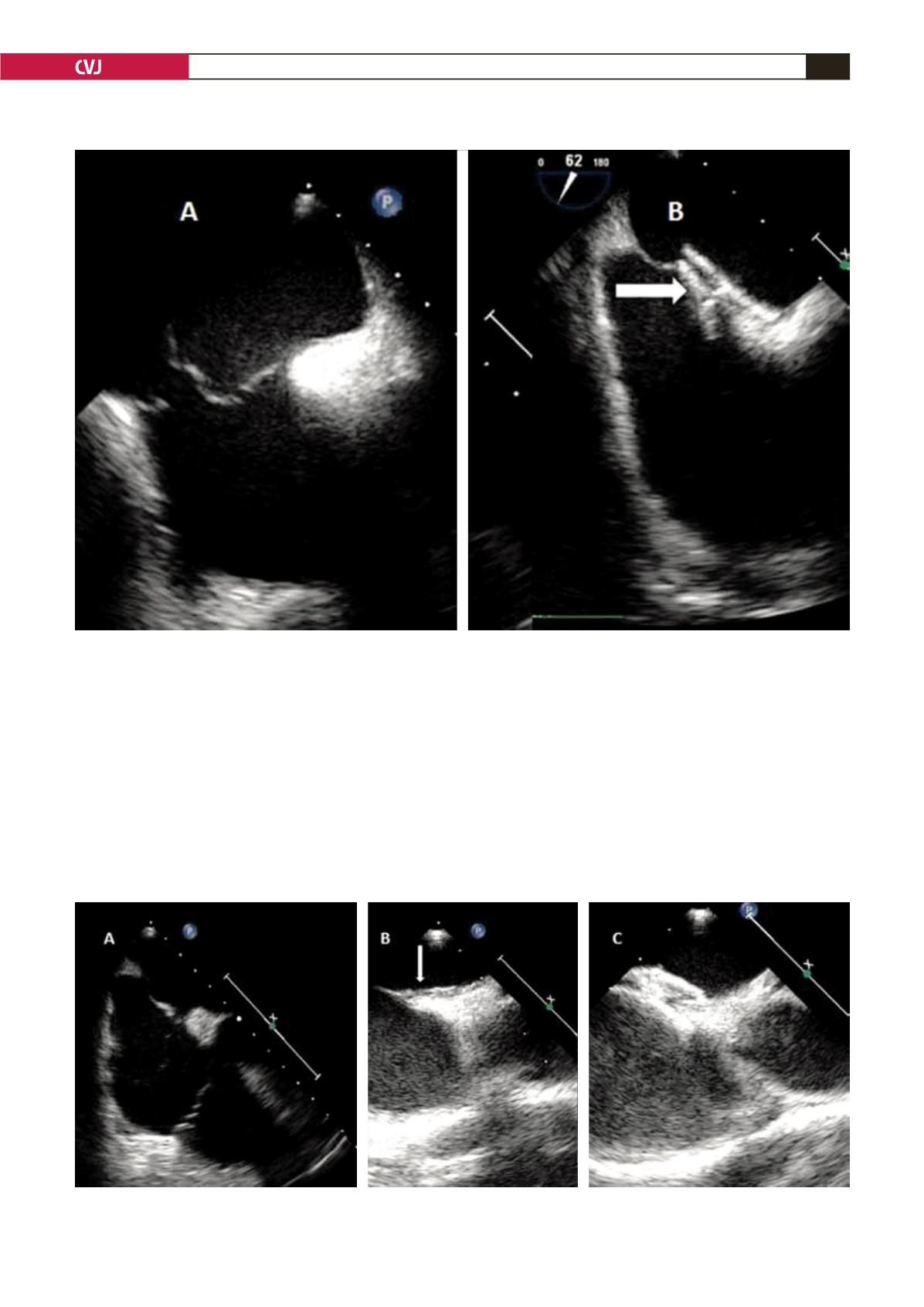
Fig. 1. TEE before and after PFO closure in Patient 1. A: PFO and ASA. Multiple small defects are present. Prominent
Eustachian valve can be seen. B: Arrow indicates the device in position on the interatrial septum and stabilisation of
the ASA. Note the low profile of the device and stabilisation of the interatrial septum.
Fig. 2. TEE before and after PFO closure in Patient 1. A: PFO in the four-chamber view showing redundant interatrial
septum. B: Tunnel-like nature of PFO on a 70-degree view (arrow). C: The device in position.
CARDIOVASCULAR JOURNAL OF AFRICA • Vol 22, No 5, September/October 2011
AFRICA
275
TEE was performed in both patients six months after placement
and showed good positioning of the devices and no residual
shunting.
for closure exist. The American Heart Association, American
Stroke Association and the American College of Cardiology
Foundation therefore, in a statement, called on physicians to
consider participation in currently ongoing prospective trials in
Fig. 1. TEE before and after PFO closure in Patient 1. A: PFO and ASA. Multiple small defects are present. Prominent
Eustachian valve can be seen. B: Arrow indicates the device in position on the interatrial septum and stabilisation of
the ASA. Note the low profile of the device and stabilisation of the interatrial septum.
Fig. 2. TEE before and after PFO closure in Patient 1. A: PFO in the four-chamber view showing redundant interatrial
septum. B: Tunnel-like nature of PFO on a 70-degree view (arrow). C: The device in position.
TEE was performed in both patients six months after placement
and showed good positioning of the devices and no residual
shunting.
Discussion
PFO closure in patients with ischaemic stroke and those with
migraine remains controversial.
13-15
This can be attributed to the
fact that most studies of device closure for these patients are
observational in nature, as well as the overall lack of randomised
controlled clinical trials. As a direct r sult, no clear guidelines
for closure exist. The American Heart Association, American
Stroke Association and the American College of Cardiology
Foundation therefore, in a statement, called on physicians to
consider participation in currently ongoing prospective trials in
order to resolve these issues.
16
This is the first reported use of the Cardia
©
PFO device in
South Africa. The Atriasept™ II PFO occluder is a self-expand-
able, double-disc device with a skeleton of nitinol wires, each
covered with a polyvinyl-alcohol membrane and is available in
s zes f 20, 25, 30 and 35 mm. The two discs are linked by a
self-c ntring mechanism, which allows some angulation of each
Fig. 1. TEE before and after PFO closure in Patient 1. A: PFO and ASA. Multiple small defects are present. Prominent
Eustachian valve can be seen. B: Arrow indicates the device in position on the interatrial septum and stabilisation of
the ASA. Note the low profile of the device and stabilisation of the interatrial septum.
Fig. 2. TEE before and after PFO closure in Patient 1. A: PFO in the four-chamber view showing redundant interatrial
septum. B: Tunnel-like nature of PFO on a 70-degree view (arrow). C: The device in position.
,


