CARDIOVASCULAR JOURNAL OF AFRICA • Vol 23, No 1, February 2012
AFRICA
e11
Case Report
A mysterious case of fatal embolism after the repair of
tetralogy of Fallot: secondary to arrhythmia?
CY KARABAY, A GÜLER, A KILICGEDIK, SM AUNG, A KALAYCI, G SAHIN, IH TANBOGA, C KIRMA
Abstract
Tetralogy of Fallot (TOF) is a common cyanotic congenital
heart disease. The most important late complications observed
after repair of TOF are atrio-ventricular arrhythmias and sudden
cardiac death. We present a rare case of fatal embolism and
sudden cardiac death in a 36-year-old patient, 30 years after the
operation for TOF.
Keywords:
fatal embolus, tetralogy of Fallot, sudden cardıac
death
Submitted 24/5/10, accepted 26/11/10
Cardiovasc J Afr
2012;
23
: e11–12
DOI: 10.5830/CVJA-2010-095
Tetralogy of Fallot (TOF) is the most common cyanotic heart
disease beyond infancy, accounting for 10% of all congenital
heart malformations.
1
Despite the improved survival rate with
modern surgery, sudden cardiac death (SCD) has been recog-
nised as a devastating late complication after repair of TOF. The
prevalence of SCD in large follow-up studies varies from 2.0 to
8.3%.
2,3
Many risk factors for SCD have been determined. We
present a case of embolism localised in the brachiocephalic trunk
and left axillary artery, possibly due to arrhythmia that developed
30 years after TOF repair.
Case report
A 36-year-old male patient was brought to our clinic after 30
minutes of resuscitation at home by an emergency team. He
was under inotropic support, and had a blood pressure of 75/50
mmHg. His surface ECG showed normal sinus rhythm with a
QRS duration of 110 ms.
He had had an operation for TOF at six years of age but had
failed to appear for routine follow up in the last 10 years. It was
also learned that he had experienced palpitations for a week
before the event. He had suffered from abrupt severe pain in
both arms and had become unconscious on the day of the event.
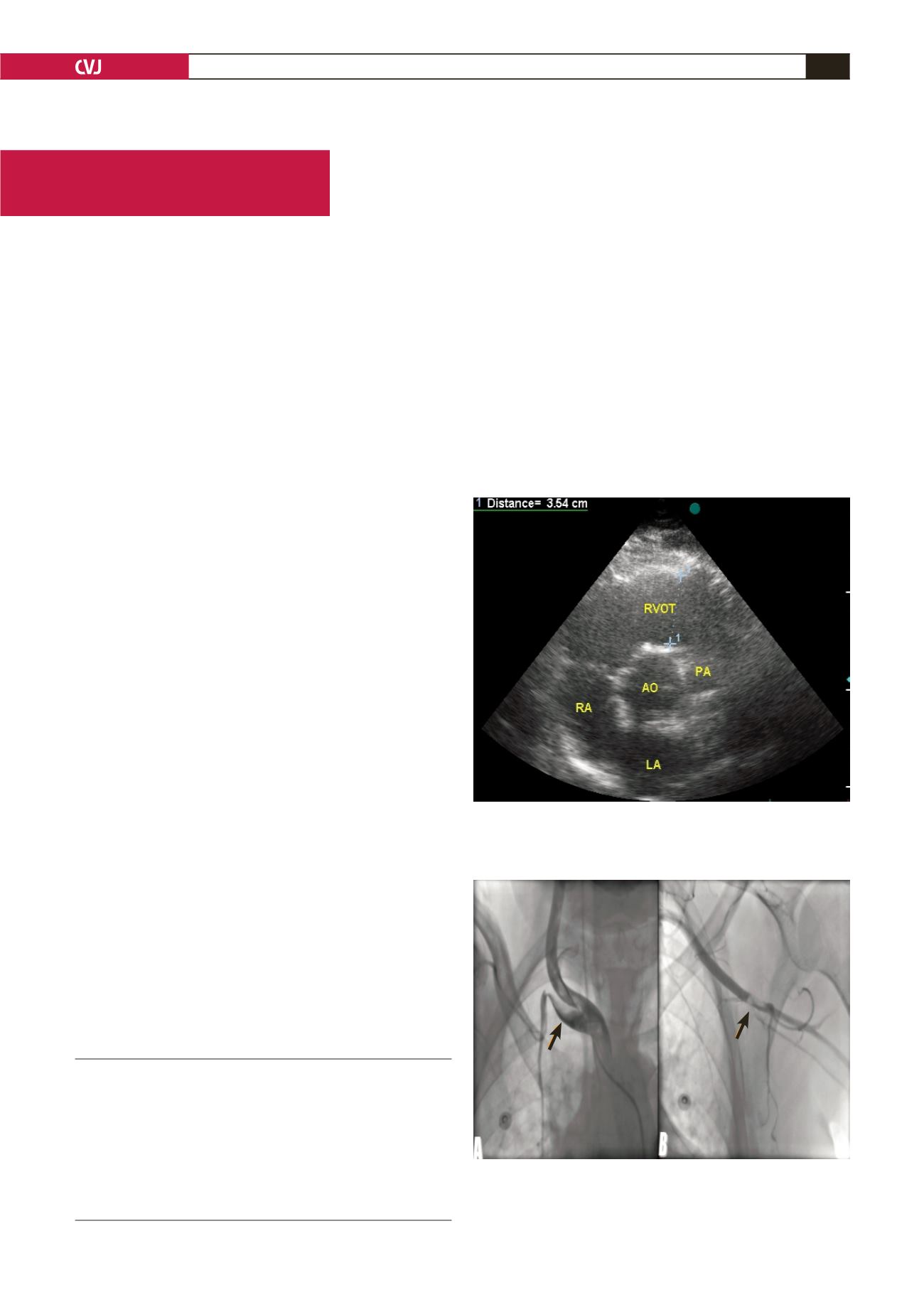
Transthoracic echocardiography (TTE) was done to rule out
aortic dissection. On TTE, a left ventricular ejection fraction of
48% (by Simpson’s method), moderate pulmonary regurgitation
and enlargement in the right ventricular outflow tract (RVOT)
(Fig. 1) were found.
Cardiology Clinic, Kartal Kosuyolu Heart and Research
Hospital, Istanbul, Turkey
CY KARABAY, MD,
A GÜLER, MD
A KILICGEDIK, MD
SM AUNG, MD
A KALAYCI, MD
G SAHIN, MD
IH TANBOGA, MD
C KIRMA, MD
Fig. 1. Enlargement in the right ventricular outflow tract
(RVOT) secondary to moderate pulmonary regurgitation.
RA: right atrium; LA: left atrium; RVOT: right ventricular
outflow tract; PA: pulmonary artery; AO: aorta.
Fig. 2. A. Thrombus extending from brachiocephalic
trunk to the right subclavian artery and the right common
carotid artery (arrow). B. Thrombus in the left axillary
artery (arrow).


