CARDIOVASCULAR JOURNAL OF AFRICA • Vol 24, No 4, May 2013
e14
AFRICA
She was transferred to the cardiac catheterisation laboratory
to perform emergency coronary angiography, which revealed a
severe stenosis of the LMCA, together with diffuse atherosclerotic
lesions of varying degrees in the left anterior descending (LAD)
coronary artery. The left circumflex coronary artery (LCX) and
right coronary artery were free of clinically significant disease
(Fig. 3). The patient was transferred to the operating room for
emergency coronary artery bypass grafting (CABG) and the
surgery was performed successfully.
The pre-operative cardiac troponin level was
>
50 ng/ml and
gradually decreased after CABG. Blood tests performed one
week after surgery revealed the presence of severe dyslipidaemia
[total cholesterol 797 mg/dl, high-density lipoprotein (HDL)
cholesterol 127 mg/dl, low-density lipoprotein (LDL) cholesterol
599 mg/dl].
She recovered well and was extubated on the first day post-
operatively. She was started on atorvastatin, acetylsalicylate,
clopidogrel and meteprolol, and discharged uneventfully on day
eight.
Discussion
Peripartum myocardial ischaemia is a different entity because
the underlying cause is not usually atherosclerosis, in contrast
to ischaemic disease in the older population.
6
Factors such as
increasing maternal age, increasing rates of maternal obesity,
smoking, diabetes mellitus and hypertension are possible
contributors to the rise in frequency of pregnancy-associated
AMI.
7
Coronary atherosclerotic lesions have been reported in only
20–43% of pregnancy-related AMIs.
2,5
Risk factors for coronary
artery disease in pregnancy are similar to traditional risk
factors observed in the general population. More common
cardiac risk factors in young women include a family history
of atherosclerotic disease, dyslipidaemia, diabetes mellitus,
cigarette smoking and previous use of oral contraceptives.
Dyslipidaemia may be worsened during pregnancy because HDL
cholesterol is significantly decreased during gestation.
8
Spontaneous coronary dissection is a rare event, observed
in only 15% of cases and often associated with haemodynamic
stress during labour. Such spontaneous dissection is most often
encountered in fairly young,
9,10
otherwise healthy women, with
approximately 30% of cases occurring in late pregnancy (near
term) or within three months postpartum. Coronary dissection
most commonly affects the left main coronary artery, the left
anterior descending artery or both.
9,11,12
This causes extensive
ischaemia or thrombosis/infarction or both, which can precipitate
severe haemodynamic compromise with a high risk of maternal
and foetal adverse outcomes.
13
Possible causes of coronary spasm include enhanced vascular
reactivity to angiotensin II and norepinephrine, and endothelial
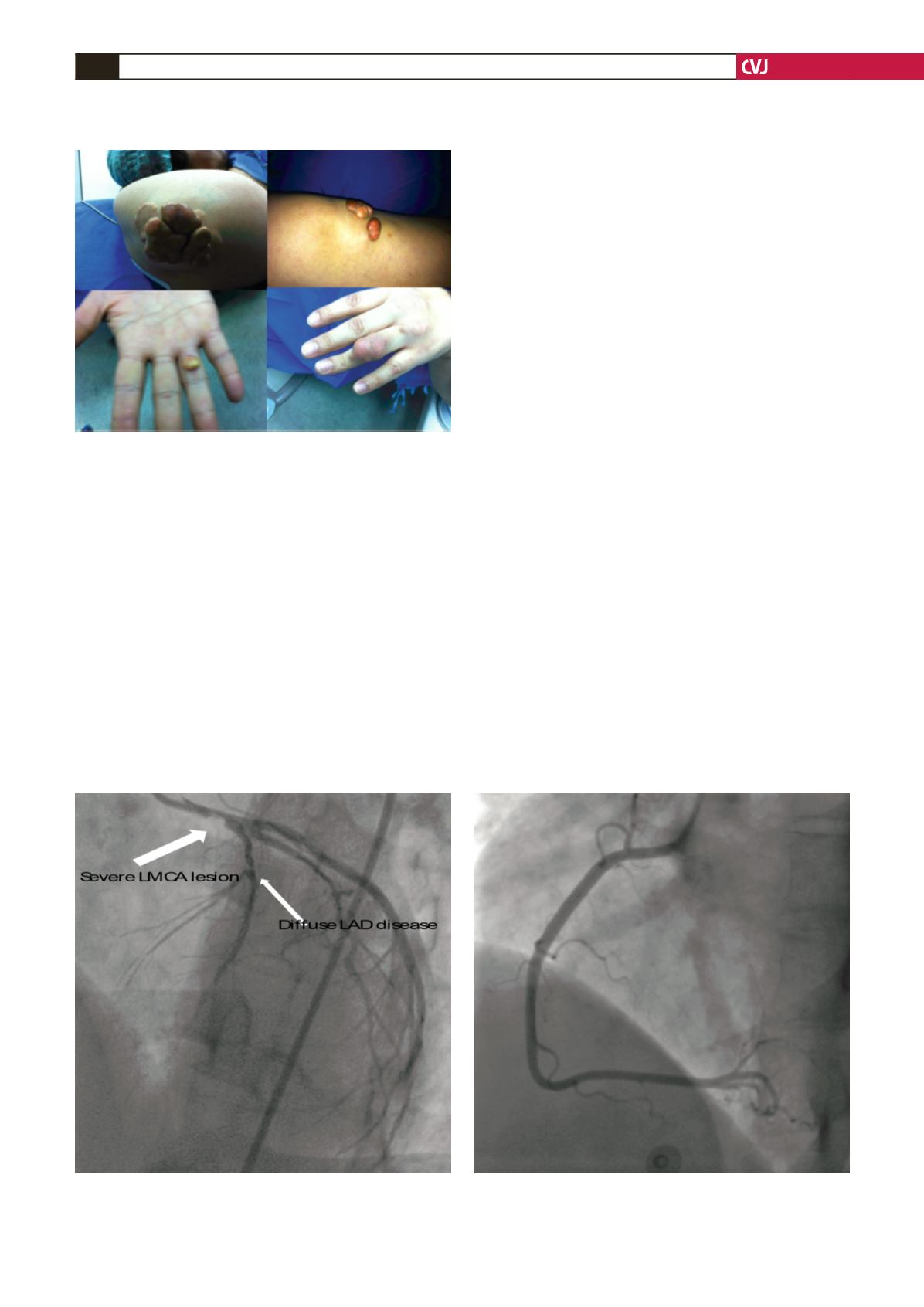
Fig. 2. Eruptive xanthomas on the skin of the elbow
(vegatative), knee and both ring fingers.
Fig. 3. The left anterior oblique cranial projection shows a severe atherosclerotic lesion in the left main coronary
artery (thick arrow) and diffuse atherosclerotic disease of the left anterior descending artery (thin arrow). A normal
left circumflex and right coronary artery is seen. LMCA: left main coronary artery, LAD: left anterior descending artery.


