CARDIOVASCULAR JOURNAL OF AFRICA • Vol 24, No 4, May 2013
AFRICA
e11
Pericardial fluid was then evacuated through the pigtail
catheter but approximately 100 to 200 ml of fluid was left within
the pericardium to provide a measure of safety. The pigtail
catheter was then removed and a 12-F dilator was advanced over
the guide wire.
A self-positioning catheter, the Inoue balloon catheter set
(Shineyard Medical Device Co. Ltd, Shenzhen, China) at 22
mm was exchanged over the guide wire and advanced into the
pericardial space. The distal portion of the balloon was inflated
first and the catheter was then pulled back gently until the distal
balloon anchored itself at the parietal pericardium (Fig. 2). The
balloon was then rapidly inflated to its full extent until the waist
disappeared (Fig. 3). Three inflations were performed to ensure
adequate tearing of the pericardium. After this procedure, 10 to
15 ml of contrast medium was rapidly injected to determine the
exit of free fluid (Fig. 4).
We performed an echocardiography at the end of the procedure
(Fig. 5). After draining the pericardial fluid, a drain was left in
place until the next day (as long as less than 100 ml was drained
over the next 24 hours).
Results
In all patients, the procedure was successful in a single session
with one pericardial puncture. A sufficient opening was obtained
by inflating the balloon at least three times. There were no later
recurrences of pericardial effusion. In all cases, the pericardial
fluid was bloody and varied in volume from 750 to 1 200
ml. Almost complete evacuation of the pericardial effusion
was achieved in all patients. There were no post-procedure
complications in any of the patients.
During the four to six months of follow up, all patients were
alive. Massive pericardial effusion and pericardial tamponade
did not recur in any of the patients. In two, we found minimal
pericardial effusion. The patients did not re-admit to the hospital
for symptoms related to the pericardium and showed no signs of
constrictive pericarditis.
Discussion
The incidence of recurrent pericardial effusion after
pericardiocentesis is 15 to 40%, according to different authors.
1,4,5
In patients with recurrent large pericardial effusions or failed
pericardiocentesis, two surgical options have been described:
creation of a pericardial window through a subxiphoid approach
or via a thoracotomy, followed by pericardiectomy.
The subxiphoid pericardial window has been the surgical
option of choice during the last few years due to its high rate of
success (91%) and low incidence of complications.
2,3
Despite this,
because patients withmalignancies are frequently undernourished
and in poor general condition, any kind of surgical approach has
an increased risk of peri-operative complications.
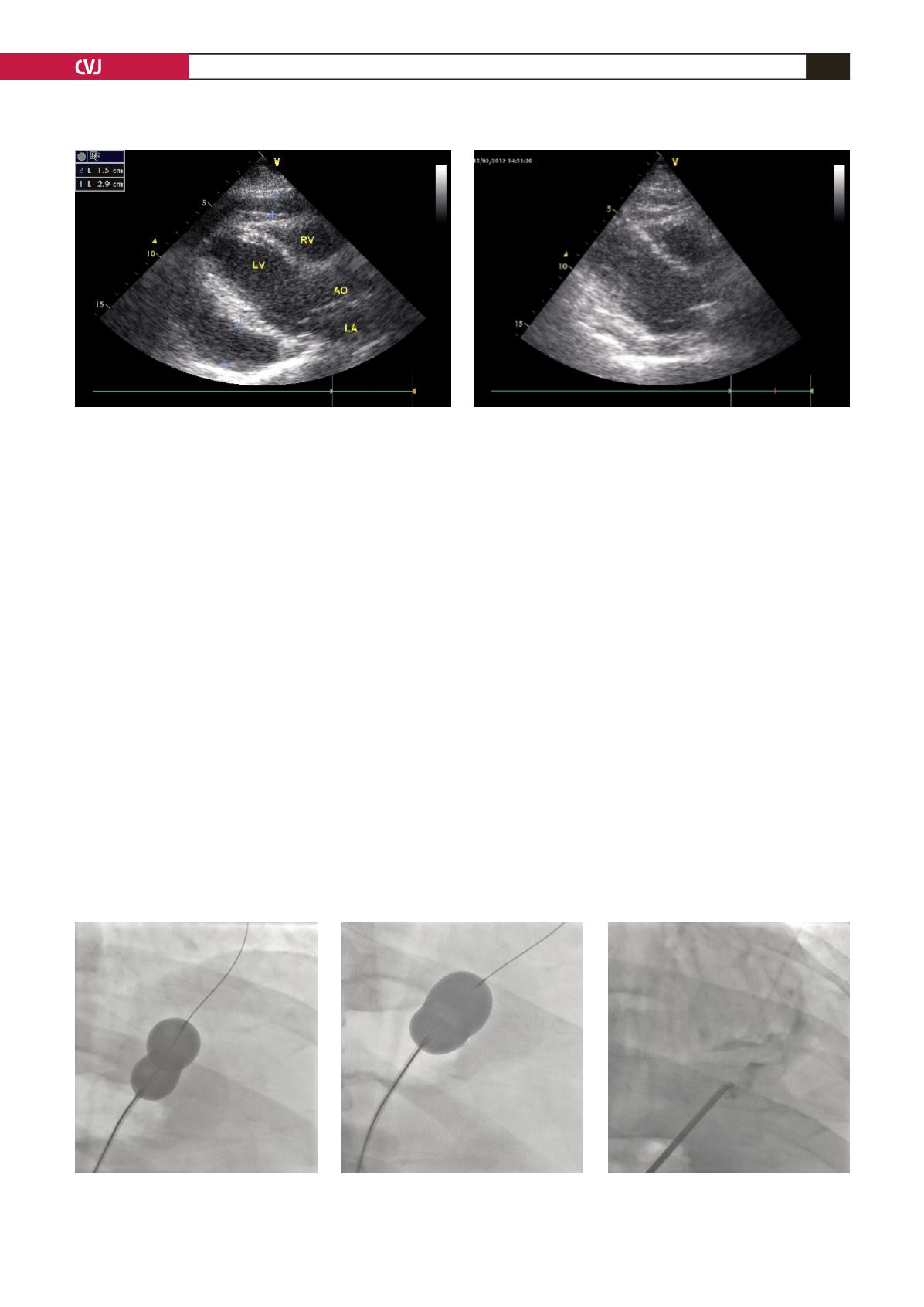
Fig. 1. The echocardiographic signs of cardiac tamponade.
Fig. 4. Contrast medium was washed
out from the pericardial space.
Fig. 2. The distal portion of the
balloon was inflated first.
Fig. 3. The balloon was rapidly inflat-
ed to its full extent until the waist
disappeared.
Fig. 5. Echocardiography after the procedure.


