CARDIOVASCULAR JOURNAL OF AFRICA • Vol 24, No 5, June 2013
AFRICA
195
Africa are urine glucose, random blood
glucose (dependant on the population-
specific threshold), fasting plasma
glucose, glycated haemoglobin, point-of-
care capillary glucose, and 75- and 50-g
oral glucose tolerance tests.
Lifestyle interventions remain the first
consideration in the prevention and treat-
ment of diabetes. Weight control, healthy
eating and physical activity levels are
strong determinants of disease progres-
sion. Drug affordability and availability
are limiting factors in the medical manage-
ment of diabetes. Monitoring and surveil-
lance of complications and the treat-
ment of complications and co-morbidities
are essential to long-term diabetes care
(Fig. 1).
2
1.
Said Norou Diop. Management of diabetes
in Africa.
2.
Andre Kengne. The appropriate public
health response to the rise of obesity and
diabetes in Africa.
3.
Terence Forrester. The role of nutrition and
early life influences on the pathogenesis
and prevention of cardiometabolic diseases
in Africans.
Sickle cell disease: an update on
the CADRE study
Sickle cell disease (SCD), also known
as sickle haemoglobin and haemoglobin
S, is an inheritable disorder resulting in
sickling of red blood cells and chronic
haemolysis. Haemoglobin has two subunit
chains, alpha and beta, with the normal
referred to as HbA. In SCD, the alpha-
chain is normal but abnormal versions
of beta-globin (e.g. HbS and HbC) are
present. This results in a characteristic
modification of the smooth doughnut
shape of the red blood cell into a crescent
shape. Cells then lack plasticity and can
block small blood vessels, impairing
blood flow. Shortened red blood cell
survival also leads to subsequent anaemia.
Acute complications of SCD include
vaso-occlusive pain (blood flow block,
can occur anywhere but most commonly
arms, legs, chest and spine) and chest
syndrome (often occurs suddenly and can
be life-threatening, resembles pneumonia,
multiple episodes can cause permanent
lung damage). Chronic vascular events
include stroke, pulmonary hypertension,
cardiac disease, nephropathy, retinopathy,
leg ulcers and osteonecrosis.
Different types of SCD vary in sickle
symptoms and disease severity, dependant
on the inherited mutation.
•
HbAS individuals carry the trait but
usually display no signs and symptoms
of disease.
•
HbSS is the most common and severe
form of SCD, with a variety of symp-
toms and complications.
•
HbSC presents mild to moderate
complications.
•
HbS-beta-thallasaemia comes in two
forms: beta0 and beta
+
, with a broad
range of symptoms and severity.
•
Other forms.
Of children born with SCD, 90% are
born in sub-Saharan Africa, implying a
prevalence of greater than 25 million.
Yet SCD data predominantly arises out
of America and Europe, with very small
studies of less than 250 patients.
CADRE is a multinational cohort for
the study of SCD chronic vascular events
in Africa. Study sites are in Senegal, Mali,
Cote d’Ivoire, Cameroon and Gabon.
Among the objectives of this first SCD
multinational cohort is to build up the
world’s largest database of 4 500 SCD
patients, to assess the prevalence of the
main chronic micro- and macrovascular
complications of SCD in Africa and
to look for associations between these
main complications, arterial stiffness and
haematological parameters.
Clinical investigations of the study
include socio-economic data, medi-
cal history and clinical examination.
Functional investigations include echo-
cardiography and pulse-wave velocity
(PWV) measurements. Biological inves-
tigations include urine proteins and urine
creatinine, blood creatinine, blood cell
count and haemolysis markers.
Current CADRE results give evidence
of two main SCD populations: SS,
Sbeta0, SC and Sbeta
+
. In SCD patients
carotid–femoral PWV
=
7.8 (7.0–8.8) m/s
versus 9.5 (8.4–10.7) in controls, even
after adjustment for gender, age, blood
pressure and BMI. The more severe SCD
phenotypes (SS and Sbeta0) have lower
PWV than others (SC and Sbeta
+
), even
after adjustment for age, blood pressure
and haemoglobin. Multivariate analysis
indicates that PWV is independently
correlated with age (
p
<
0.001), blood
pressure (
p
<
0.001) and haemoglobin (
p
=
0.01). However, PWV is not correlated
with LDH or bilirubin levels (haemolysis
markers).
The CADRE study provides valuable
data on the incidence of chronic vascular
‘The omission of cardiovascular
disease from the Millenium
Development Goals has cost us years
of action and millions of lives’.
Vash-Mungal Singh, South Africa
‘A mountain of information emerg-
ing from our scientists on the African
continent alerts us to a looming crisis.
This is an important opportunity for
scientists to report on disturbing
trends with resgard to cardiovascular
disorders in Africans.’
Samuel Omokhodion, Nigeria
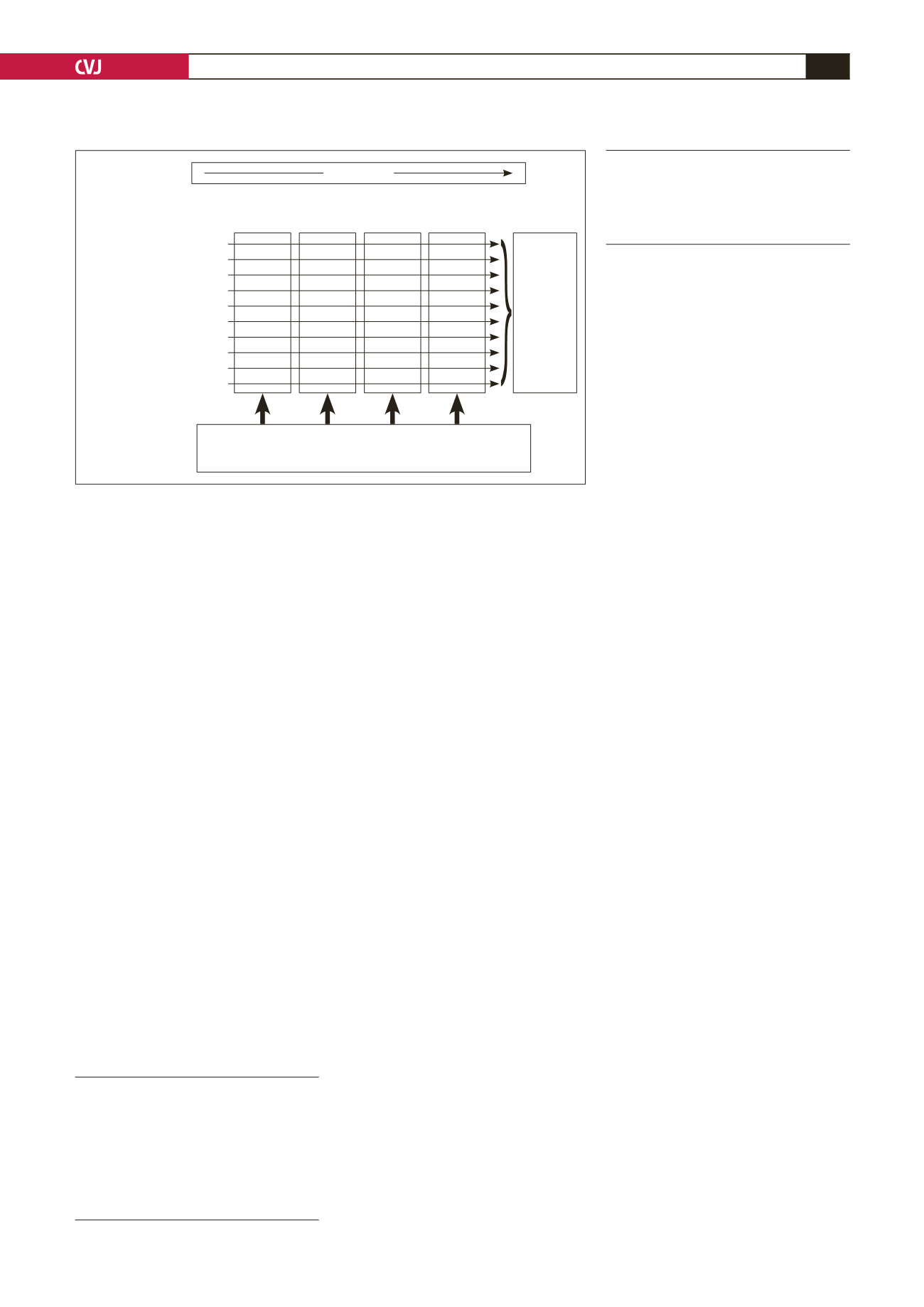
Fig. 1. Lifecourse perspective to chronic disease prevention.
2
Health promotion and
protection strategies (eg)
Mothers
and Infants
Younger
people Adults
Older people/
elders
Healthy eating
Active living
Tobacco control
Safe alcohol use
Mental health promotion
Substance abuse prevention
Sexual health
Immunisation
Injury prevention
Environmental health
Integrated approaches based on key settings: eg health-promoting
schools, primary healthcare, “well-person” clinics, healthy
workplaces, healthy literacy, community capapcity building
Lifecourse
Health
outcomes
•
•
National
health
priorities
areas
•
•
Others


