CARDIOVASCULAR JOURNAL OF AFRICA • Vol 24, No 5, June 2013
AFRICA
e9
The radiologist, cardiovascular surgeon and cardiologist
re-examined the CT images due to remaining uncertainty. The
radiologist was adamant about the radiological diagnosis and
emphasised there were no typical signs of a dissection flap.
However he agreed on second review that there was a faint intra-
aortic double line in the short segment of the ascending aorta
just above the valves but it seemed more like an artifact than an
intra-aortic flap.
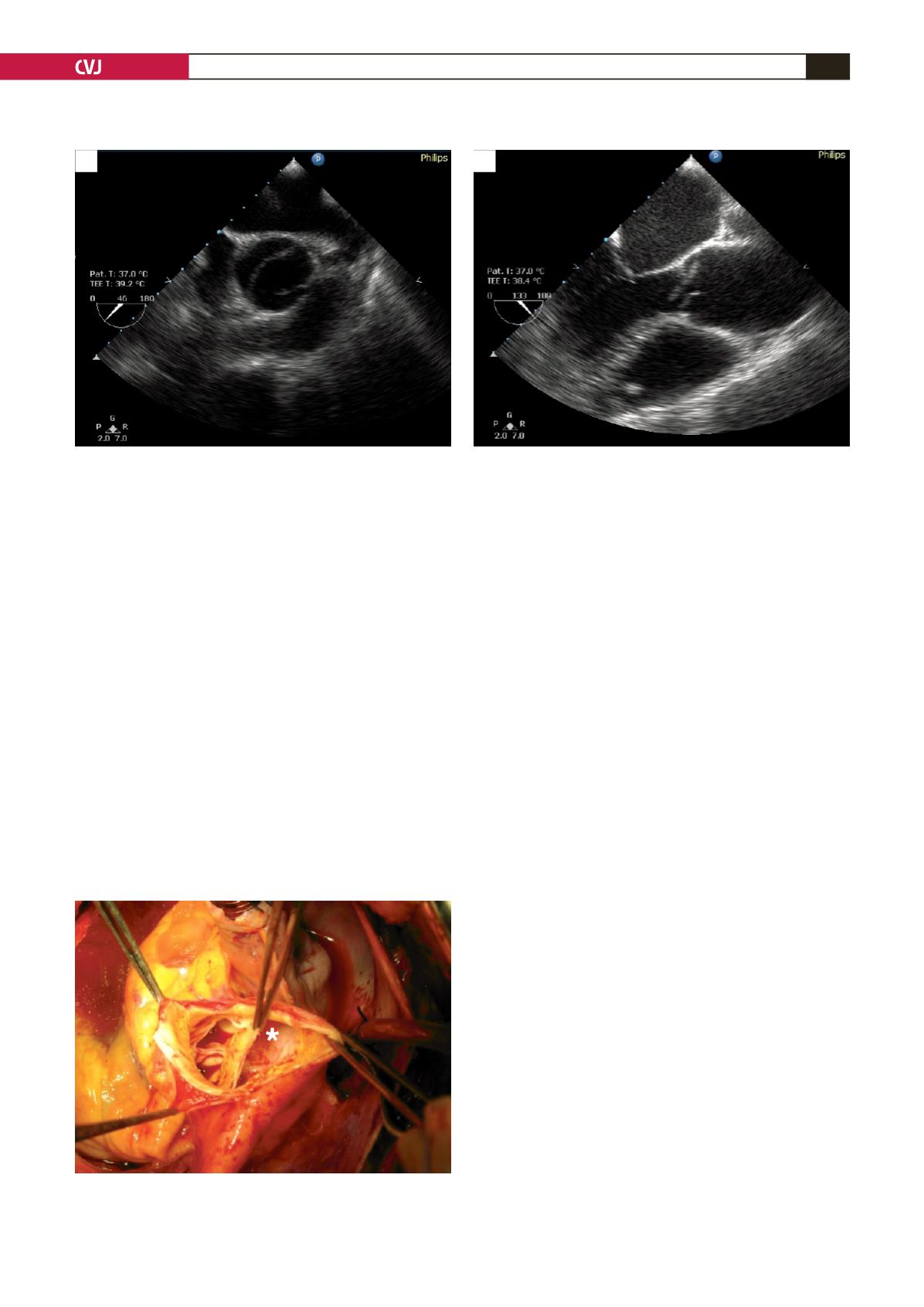
Due to uncertainty, the patient was sedated and
transoesophageal echocardiography (TEE) was performed. TEE
demonstrated an accessory valve-like structure in the ascending
aorta, 2 cm above the bicuspid aortic valves (Fig. 2A, B). There
was severe aortic valve insufficiency. It was reported to be an
atypical form of aortic dissection.
The patient was scheduled for aortic valve and ascending
aorta replacement. During the operation, the dilated aortic
root and proximal ascending aorta were observed but the
distal ascending and arcus aorta were in normal alignment.
There was a retrograde spiral dissection of the ascending aorta
(approximately 270 degrees of the circumference of the aorta
was involved) with an entry tear 2 cm above the coronary ostia,
extending to the proximal aortic root (Fig. 3). The aortic wall was
secure at the distal part of the ascending aorta.
The aortic valve and proximal ascending aorta were resected
and a modified Bentall procedure was performed using a 25-mm
composite graft. The patient had no complications and was stable
four months after the procedure.
Discussion
Dilation of the ascending aorta in children with bicuspid
aortic valves has been previously described in some cohorts
of children.
9,10
Moreover, adults with bicuspid aortic valves
are shown to be at greater risk for progressive aortic dilation
independent of valve function.
11
The exact reason is unknown
but there are some suggested physiopathological mechanisms.
The neural crest is a remarkable structure. Some studies
have shown that the neural crest plays an important role
in the development of cardiac and a variety of non-cardiac
structures. The cardiac structures derived from the neural
crest involve the outflow tract of the heart and the aortic arch
system. Mal-development of neural crest cells are thought to
be responsible for the combined occurrence of outflow tract
(e.g. bicuspid aortic valve), aortic arch (e.g. coarctation) and
non-cardiac anomalies.
12
Of interest, another important study demonstrated a strong
association between endothelial nitric oxide synthase (eNOS)
deficiency and the presence of a bicuspid aortic valve.
13
They
reported that mice lacking functional eNOS demonstrated a high
incidence of bicuspid aortic valves.
This evidence suggests that a patient with a bicuspid valve
should be carefully monitored for aortic pathologies. Atypical
forms of aortopathies such as spontaneous retrograde dissections
may occur, and both clinicians and radiologists should be on the
alert. Diagnosis may require more accurate examination.
Conclusion
It appears that the transesophageal echocardiogram is the
gold standard of diagnostic procedures in cases of retrograde
Fig. 3. Intra-operative view showing the entry tear of the
dissection flap in the distal part of the ascending aorta
(asterisk). Note the bicuspid aortic valves.
Fig. 2. A. Transoesophageal echocardiography depicting the bicuspid aortic valve. B. Transoesophageal echocardiog-
raphy demonstrating an accessory valve-like structure 2 cm above the aortic valves. Findings were suggestive of an
atypical form of aortic dissection in the patient with a bicuspid aortic valve.
A
B


