CARDIOVASCULAR JOURNAL OF AFRICA • Vol 24, No 5, June 2013
e12
AFRICA
amiodarone upon detection of ventricular tachycardia (VT) on
electrocardiography (ECG) (Fig. 1).
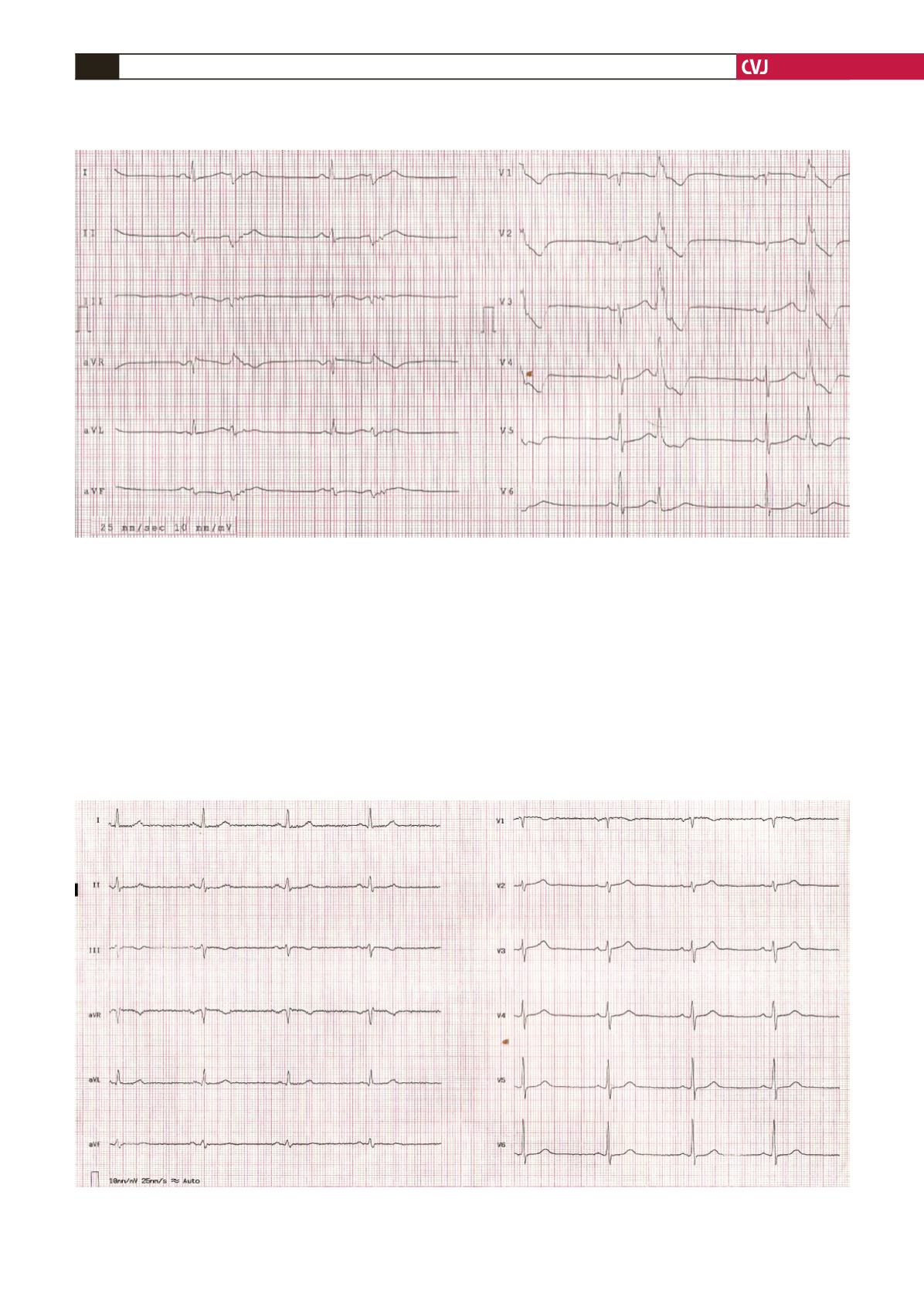
At the first admission to our hospital, the patient had a normal
sinus rhythm with ventricular bigeminy extrasystole, and her
corrected QT (QTc) interval was measured at 0.53 seconds on
ECG (Fig. 2). She had no relevant family history and no cardiac
risk factors, except for hypertension. She had no coronary artery
disease, according to a coronary angiography performed seven
months earlier.
We learnt the reason for the coronary angiography had been
for atypical exertional chest pain. The patient had previously
used bisoprolol 5 mg, valsartan 160 mg and amlodipine 10 mg
for hypertension. In addition, she had received ibandronic acid
treatment for osteoporosis for two weeks.
During the physical examination, the patient’s blood pressure
and cardiac pulse rate were 129/62 mmHg and 63 beats/min,
respectively. No pathological sound was heard during pulmonary
and cardiac auscultation. Serum potassium, calcium and
magnesium levels and other routine biochemical measurements
were in the normal ranges. No significant increase was detected
during cardiac enzyme monitoring, so VT associated with
coronary ischaemia was not a primary consideration.
Fig. 2. Normal sinus rhythm with ventricular bigeminy extrasystole and prolonged QT interval, measured as 0.53
seconds, after medical cardioversion.
Fig. 3. Corrected QT interval returned to normal, measured as 0.42 seconds, two weeks after discontinuation of iban-
dronic acid.


