CARDIOVASCULAR JOURNAL OF AFRICA • Volume 25, No 4, July/August 2014
178
AFRICA
In Europe, cardiovascular diseases (CVD) account for around
40% of all deaths under the age of 75 years. SCA is responsible
for more than 60% of adult deaths from ischaemic heart disease
(IHD).
2
Conversely, in young populations under 40 years,
inherited ‘arrhythmogenic’ cardiac disorders are the main cause.
8
The initial recorded rhythm in patients presenting with a sudden
cardiovascular collapse is ventricular fibrillation (VF) in 75 to
80%, whereas bradyarrhythmias and asystole are thought to
contribute to a minority of SCDs.
4,16
Rationale
The high prevalence and incidence of SCD in Western countries
have led to the recognition that SCD is a major public health
problem and the increased deployment of automatic external
defibrillators in public places.
Recent reports by the World Health Organisation (WHO)
indicated that non-communicable diseases (NCDs) are becoming
a significant cause of morbidity and mortality in African
countries.
19-26
About 50% of this burden is attributable to CVD.
27
Projections from the Global Burden of Disease project suggest
that from 1990 to 2020, the burden of CVD faced by African
countries will double and a large proportion of the victims
of CVD will be middle-aged people.
28
National public health
policies regarding detection, prevention and treatment of NCDs
are inconsistent, mainly due to lack of epidemiological data.
Regarding the magnitude of the problem, the ministers of
health and heads of delegations of the WHO African region
convened at a regional consultation on the prevention and
control of NCDs in Brazzaville and acknowledged the ever-
increasing dual burden of communicable and non-communicable
diseases in the region, and the associated disabilities and
premature deaths.
29
Almost all leading causes of SCD have been
described in Africa (Table 1). Indeed some reports of SCD in
sub-Saharan Africa have been published;
30-37
and
several studies
report conflicting data regarding the prevalence of CHD in
sub-Saharan Africa.
38-40
SCA from acute myocardial infarction is a rapidly growing
cause of morbidity and mortality among black Africans (Fig.
1). However, studies specifically targeted to provide robust data
regarding the epidemiology of SCD in Africa are warranted.
Missed diagnosis rather than misdiagnosis is a characteristic of
unexpected cardiac death in Africa.
31
The occurrence of an unexpected death in a young, otherwise
healthy individual is a devastating event for the family and
society. It is now clear that a genetic predisposition may exist and
therefore a targeted diagnostic work-up is required in subjects
resuscitated from cardiac arrest who show a structurally intact
heart. Since these approaches are often not available within the
medical system in sub-Saharan Africa and as the population is
not aware of the role of the heart in death, juvenile cases are still
often attributed in several instances to witchcraft, which prevents
the investigation of the medical causes (Fig. 2).
36,
41
The second major concern regarding SCD in Africa is the lack
of qualified personnel to accurately diagnose and manage CVD,
as well as the absence of basic diagnostic tools in many health
facilities.
42
Given these weaknesses, policies for prevention and
control of CVD are incomplete without addressing the problem of
SCD. Moreover, there is an opportunity to address these challenges
through primary prevention of SCD, secondary prevention through
the introduction of widespread cardiopulmonary resuscitation
(CPR) education efforts, and lastly, tertiary prevention through
treatment of reversible causes, as well as the dissemination of
implantable automatic cardiac defibrillators. Understanding the
epidemiology of SCD allows the introduction of a comprehensive
strategy and implementation of appropriate actions in the WHO
global agenda for the fight against NCDs.
The Pan-African Sudden Cardiac Death (Pan-African SCD)
study is a collaborative study that aims to collect comprehensive
Fig. 1.
ECG of a patient from Nigeria who died suddenly in
ICU within one hour of onset of chest pain, revealing
anterior myocardial infarction. ECG: electrocardiogram,
ICU: intensive care unit.
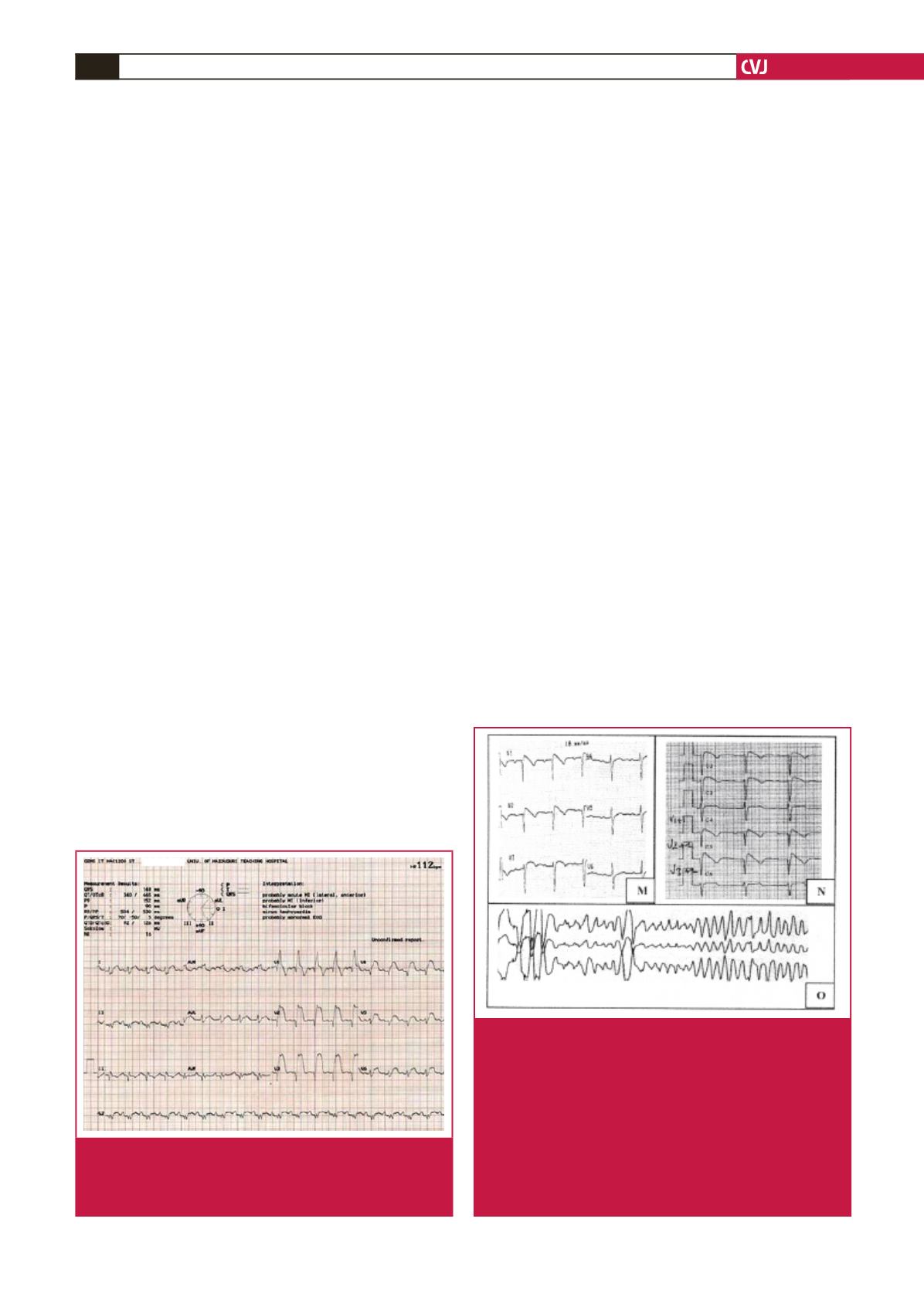
Fig. 2.
In a 45-year-old patient from Ivory Coast, syncope while
eating was managed in ICU. ECGs show spontaneous
coved-type BrS patterns in the right precordial leads
(M, N). Further, the patient experienced arrhythmic
storms treated by quinidine hydrochloride in the setting
of implantation of an ICD. Stored electrograms show
several episodes of VF (O). The patient was managed
in France, his older brother died suddenly in Ivory Coast
at age 45 years and the death was attributed to witch-
craft. ICU: intensive care unit, ECG: electrocardiogram,
BrS: Brugada syndrome, VF
=
ventricular fibrillation.


