


















 48 / 74
48 / 74

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 25, No 5, September/October 2014
242
AFRICA
increased use of EVAR for not only straightforward cases
but for those with more complex and challenging aneurysm
anatomies. The tips and tricks presented in this report regarding
Endurant™ trapped delivery systems should prove especially
useful for procedures involving adverse proximal aortic necks
and iliac anatomies. It is important to remember that hostile
infrarenal aortic aneurysm anatomy such as a very short, severely
angulated or dilated proximal neck still remains a major cause of
early failure of EVAR and jeopardises long-term efficacy.
Introduction of new endograft devices into the vascular
realm will most likely expand the indications for procedures
once considered not feasible in the past. Anatomical morphology
and measurements of the aneurysm will be crucial to device
selection, and device choice critical to the successful positioning
and adaptation of the stent-graft to the aneurysm environment
for its exclusion from the circulation.
The Endurant
TM
stent-graft is part of a next-generation
system that was designed with the clear intention of expanding
the applicability of EVAR for AAA. Initial clinical experience
has demonstrated that it can be used in challenging anatomies
and can be delivered and deployed safely, even in highly
angulated (> 60°) and short (< 15 mm) proximal necks.
5,6
Moreover, accruing experience suggests its safety, even in
compelling off-label indications.
7,10,12
Despite the fact that durable
efficacy of EVAR using the Endurant™ device remains to be
demonstrated, intra-operative performance of this endograft
in hostile aneurysm morphology adds valuable information to
other recently reported clinical short- and mid-term results.
5-8,10,12
Technical manoeuvres may occasionally be required in
difficult anatomies in order to avoid severe complications.
Although not confirmed in all Endurant clinical studies,
12
one
problem reported in short and tightly angulated necks is the
difficulty of retrieving the conical proximal shelter for the
non-covered proximal stent.
In a recent study, comparing the performance of the newly
released Edurant II
®
endograft in patients with friendly and
hostile infrarenal aortic anatomy eligible for EVAR, the necessity
of troubleshooting techniques was significantly higher in the
hostile group.
10
Herein, we described some of these techniques,
including those most frequently encountered, the capture of the
tip sleeve within the suprarenal bare-stent anchoring pins.
10
Its easy, accurate and controlled deployment, coupled with
its unique high flexibility and conformability contributes to
its successful use, even in severely angulated proximal necks
and/or iliac arteries. Friendly and hostile groups had equal
performance regarding all primary outcome measures, suggesting
that expanded EVAR indications can be applied with this
stent-graft.
10
Knowledge of these described troubleshooting
techniques should allow physicians to handle even the most
extreme scenarios with the Endurant
TM
endograft system and
other endoprostheses featuring a suprarenal stent with anchors
or pins.
Conclusion
The tips and tricks presented in this report should prevent or
reduce conversion to an open procedure when the Endurant
TM
delivery system becomes trapped in the suprarenal stent
anchoring pins or other graft segments. While this report is
written specifically for the Endurant
TM
device system, lessons
gleaned are applicable to similar endograft systems.
References
1.
Prinssen M, Verhoeven EL, Buth J,
et al
. A randomized trial comparing
conventional and endovascular repair of abdominal aortic aneurysms.
N
Engl J Med
2004;
351
: 1607–1618.
2.
Lederle FA, Freischlag JA, Kyriakides TC,
et al
. Outcomes following
endovascular vs open repair of abdominal aortic aneurysm: a rand-
omized trial.
J Am Med Assoc
2009;
302
: 1535–1542.
3.
Perdikides T, Georgiadis GS, Avgerinos ED,
et al
. The Aorfix stent-graft
to treat infrarenal abdominal aortic aneurysms with angulated necks
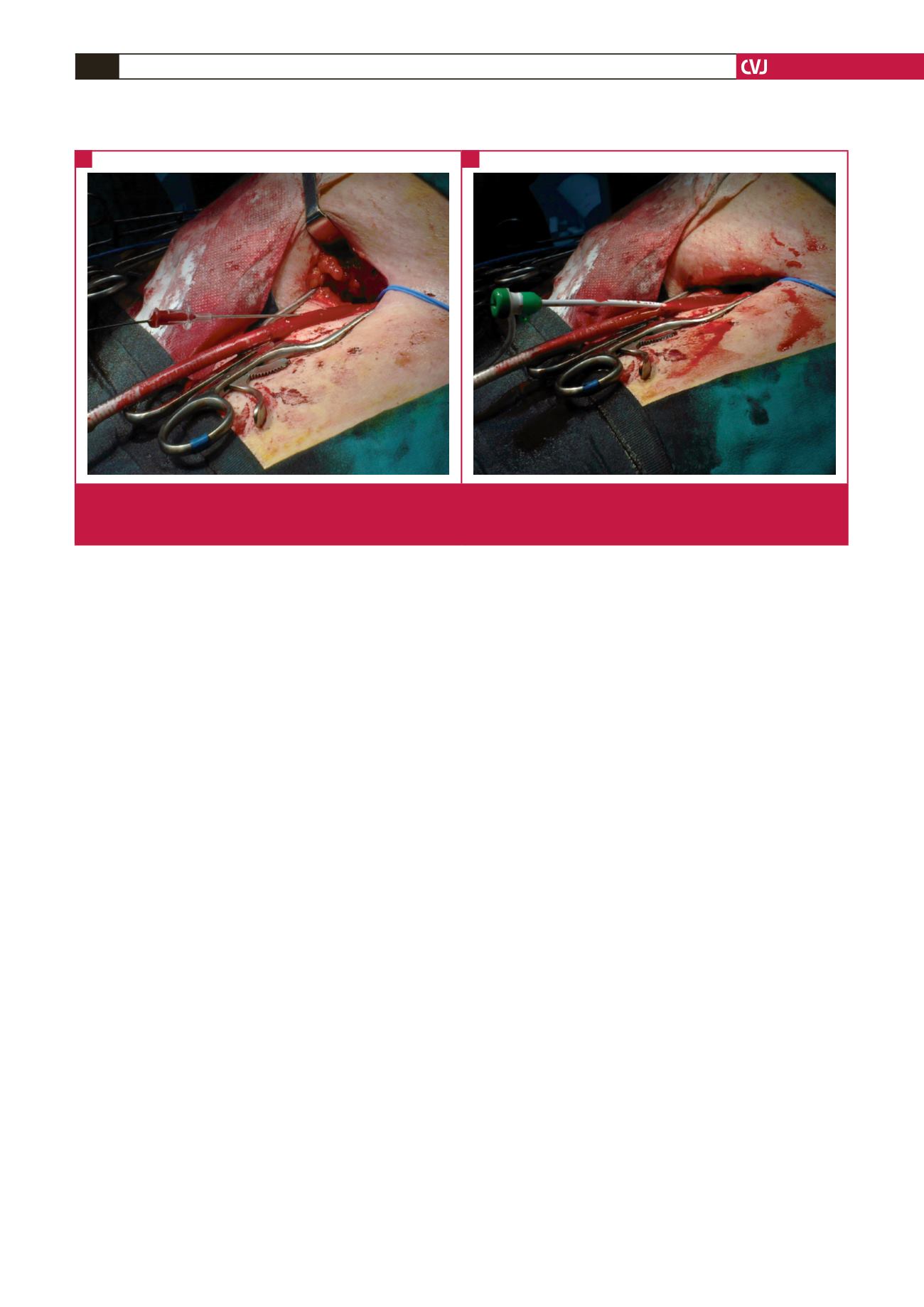
Fig. 4. Catheterisation of the delivery system in order to insert the small-diameter (4–6 mm) balloon into the external iliac artery.
Initially a guide wire is inserted through the delivery system (A), and then a short sheath (B). The next step (not shown) is
the insertion of the balloon through the sheath.
A
B