
















 48 / 64
48 / 64

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 27, No 1, January/February 2016
46
AFRICA
directed to the right and caudally. The malposition is intrinsic to
the heart and not caused by extra-cardiac abnormalities such as
right lung hypoplasia, right pneumonectomy or diaphragmatic
hernia.
2
Heterotaxy, also known as situs ambiguous, is defined as
the abnormal and disorganised arrangement of organs and
vessels within the abdominal cavity. This is in contrast to the
orderly arrangement that occurs in situs inversus or situs solitus.
Patients with situs ambiguous and dextrocardia have associated
congenital heart disease in 50 to 100% of cases, as opposed to
patients with situs solitus or situs inversus and dextrocardia.
3
The two major subcategories of situs ambiguous are situs
ambiguous with polysplenia, and situs ambiguous with asplenia.
Situs ambiguous with polysplenia (which is also known as left
isomerism or bilateral left-sidedness) is generally characterised
by a midline position of the abdominal organs and multiple
spleens/splenules. Affected patients have a lower prevalence of
congenital heart disease (50–90%) and less severe defects than
those with situs ambiguous with asplenia.
4
When evaluating a patient with dextrocardia on CT or MRI, a
systematic and sequential approach has been suggested in order to
fully evaluate abnormalities of the heart and vascular structures.
The approach favoured by Maldjian and Saric
2
is analysis of
the following in sequence: viscero-atrial situs, atrioventricular
connections, ventricular morphology, ventricular situs, chamber
positions, ventriculo-arterial connections, and relationship of the
great arteries. Finally, any associated anomalies, such as septal
defects or pulmonic stenosis, should be described.
Situs of the viscera and atria is almost always concordant, and
the atrial sinus is easily seen on cross-sectional imaging. On chest
radiograph, this is also easily assessed by the location of the liver,
spleen and stomach bubble. The morphology of the bronchial
tree (usually best assessed on CT) is more accurate in determining
atrial situs than the position of abdominal viscera. On chest
radiographs in most patients, an enlarged azygous vein can be
an indication of polysplenia, due to the high association with
azygous or hemi-azygous continuation of the inferior vena cava.
4
Evaluation of ventricular morphology, atrioventricular
connections and relationships of the great arteries usually
requires assessment by either CT angiography or MRI. The
final step in analysis involves assessment of extra-cardiac
abnormalities and possible syndromic associations. In patients
who present as adults, the possible abnormalities are limited
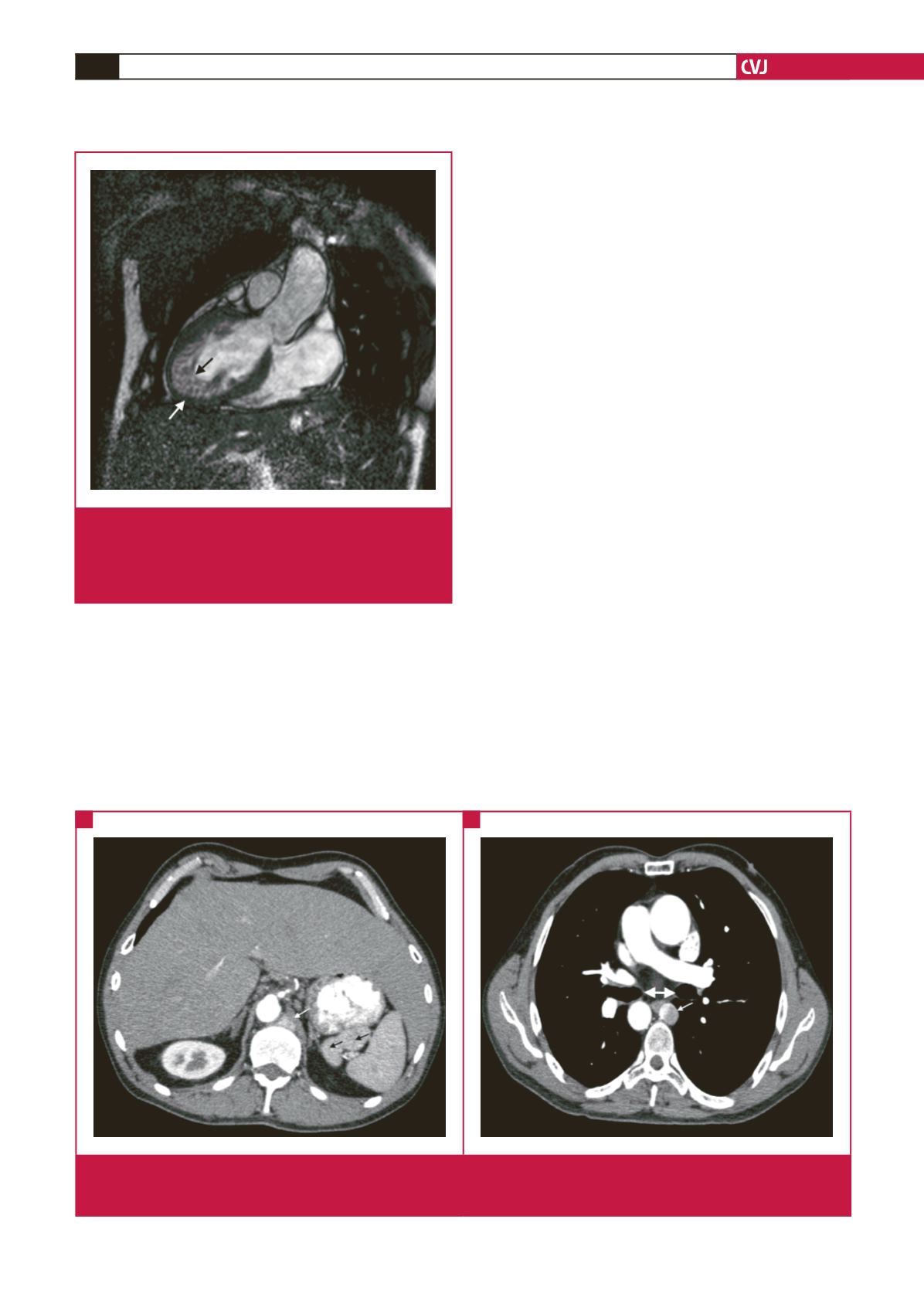
Fig. 1.
Cardiac magnetic resonance imaging (T1 bright blood
sequence) showing the dextrocardia with a midline
liver. The white arrow indicates compacted portion of
the left ventricular wall while the black arrow depicts
the left ventricular non-compaction.
Fig. 2.
Computed tomography angiogram (axial slices) showing the midline liver, absent inferior vena cava, azygous continuation
(small white arrows), multiple splenules (accessory spleens), as well as the bilateral hypo-arterial bronchi (white double
arrowheads).
A
B