
















 7 / 72
7 / 72

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 27, No 2, March/April 2016
AFRICA
61
medical certification of causes of deaths.
2
However, many cases
remain unreported due to lack of linkage to the causality of the
pregnancy.
Maternal death is rarely reported beyond six weeks
postpartum. The ICD 10 classification (version 10) defining late
maternal death (six weeks to one year) is often not applied. This
leads to the fact that death due to, for example PPCM, which
often only presents three to five months postpartum, death
due to left ventricular dysfunction and heart failure related
to hypertensive disorders in pregnancy, or death related to
right heart failure in complex congenital heart disease remains
unreported and, therefore, not adequately addressed. There is a
profound lack of knowledge on cardiac disease contributing to
morbidity and mortality, which impacts on foetal outcome, not
only in South Africa but on a global level.
The objectives of the study were to determine the
cardiovascular causes and contributing co-morbidities of
maternal death in South Africa, and to identify avoidable factors
and missed opportunities. The goal is to develop strategies to
improve quality of care, with the ultimate aim to reduce maternal
death due to cardiovascular disease.
Methods
This study was an audit of maternal deaths due to cardiovascular
disease in South Africa for the period 2011–2013. Maternal
death is defined as the death of a woman while pregnant, or
within 42 days of termination of pregnancy, irrespective of the
duration and site of pregnancy, from any cause related to or
aggravated by the pregnancy or its management, but not from
accidental or incidental causes.
3
In South Africa it is currently not a statutory requirement
to document and record late maternal deaths (up to one year
postpartum, ICD 10 code, version 10). Maternal deaths are
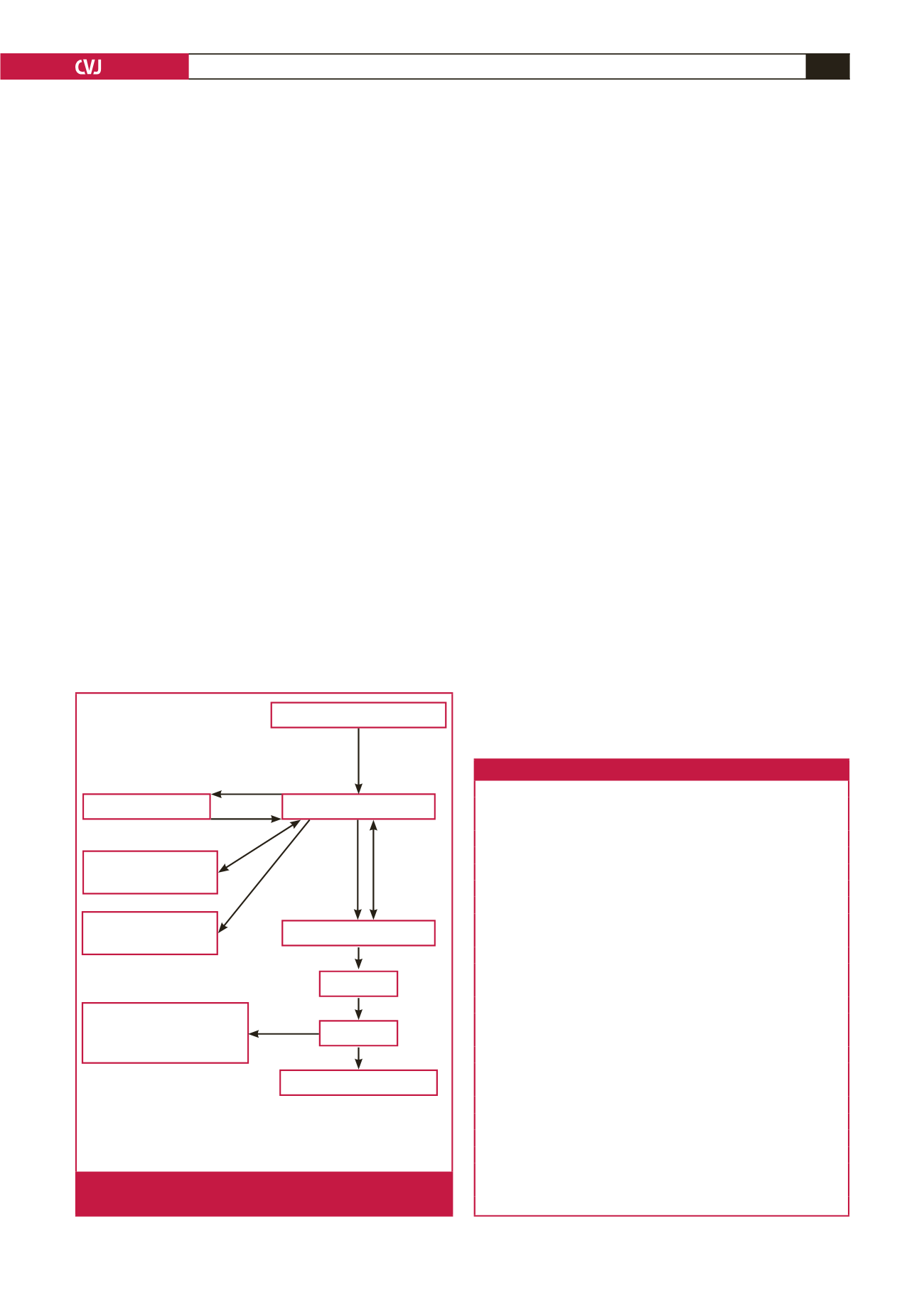
notifiable by law in South Africa. Following the death of
a mother, it is the responsibility of the clinician caring for
the mother to fill in the Maternal Death Notification form
(MDNF). This form, together with a copy of the patient’s
clinical notes, must be sent to the Provincial Maternal Child and
Woman’s Health Office within seven days of the maternal death.
Fig. 1 describes the process of the Confidential Enquiry into
Maternal Deaths.
4
One hundred and sixty-nine cases of maternal deaths related
to cardiac disease were reported to the National Committee for
the Confidential Enquiries into Maternal Deaths (NCCEMD)
and entered on the MaMMA’s database for the triennium
2011–2013. One hundred and eighteen hospital case files with
complete data were available for assessment, data extraction
and analysis. Permission was obtained from the NCCEMD and
the Department of Health of South Africa for this audit to be
conducted and presented.
Results
Overall demographic data, antenatal risk factors
and mode of delivery
The demographic information of the study population is shown
in Table 1. The majority of the women were black African, with
a mean age of 28.6 years and a parity of less than 2. More than
one-third of the patients were HIV positive. Most patients had a
low systolic blood pressure of 116
±
28.6 mmHg and an elevated
heart rate (HR).
Table 1. Demographic data of the study population (
n
=
118)
Parameters
Demographic data
Race
African,
n
(%)
104 (88.2)
Coloured,
n
(%)
7 (6.9)
White,
n
(%)
5 (3.9)
Indian,
n
(%)
2 (1.7)
Age (years)
Mean (
±
SD)
28.6 (6.49)
Range
17–43
Obstetric history
Parity median (range)
1 (1–6)
Gravidity median (range)
2 (1–6)
HIV disease status,
n
(%)
HIV positive
50 (42.4)
HIV negative
56 (47.5)
Unknown disease status
12 (10.2)
CD4 count median (SD)
275 (18-839)
Haemoglobin at presentation
Haemoglobin (g/dl), mean (
±
SD)
9.5 (1.8)
Range
5–12
Heart rate at presentation
Heart rate (bpm), mean (
±
SD)
115 (25.7)
Range
69–180
Blood pressure at presentation
Systolic blood pressure (mmHg), mean (
±
SD)
116.3 (28.6)
Diastolic blood pressure (mmHg), mean (
±
SD)
65.1 (20.7)
Maternal death
Report
completed
within 7 days
Sent
Provincial assessor
Provincial MCWH
Returned within 30 days
Death
notified
and a
unique
number
given
Provincial
assessor’s
report
sent
Anaesthetic
assessments
NCCEMD secretariat
MaMMA entry
(provincial assessor)
NCCEMD
Report
All basic data destroyed
Distributed to provinces
who distribute information
to regions and districts
MCWH: Office for Maternal Child and Women’s Health.
NCCEMD: National committee for the Confidential Enquiry into Maternal
Deaths.
MaMMA: Maternal Mortality and Morbidity database.
Fig. 1.
The process of Confidential Enquiry into Maternal
Deaths.