
















 72 / 76
72 / 76

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 28, No 2, March/April 2017
e2
AFRICA
pressure was well controlled (brachial blood pressure of 110/70
mmHg and femoral pressure of 100/65 mmHg). Prednisone
was added as oral therapy. Histopatological examination of the
aortic specimens showed a chronic inflammatory process and
eventually the final diagnosis of chronic aortitis was established.
Two-year follow-up MRI angiography and computed
tomographic (CT) examinations showed the new graft was
patent, with no abnormalities at the anastomosis sites (Fig. 2).
At the last follow up, he was asymptomatic with no neurological
dysfunction.
Discussion
Obstructive lesions or hypoplasia of the descending aorta is a rare
vascular anomaly.
1,2,4
The term middle aortic syndrome (MAS)
describes the clinico-anatomical entity of the aorta, irrespective
of its aetiology and pathogenesis. This rare pathology involves
the descending thoracic aorta, abdominal aorta or both.
3
Despite
it rarity, MAS is still the subject of clinical research, and the
aetiology of this vascular disease remains unclear.
Among other factors, non-specific aortic narrowing may be
caused by congenital influences, inflammation, developmental
disorders or infection.
2,3
MAS may be congenital or acquired
postnatally. Congenital coarctation is thought to be due to
incomplete fusion or overfusion of the embryonic dorsal
aortae. Another hypothesis implicates intra-uterine injury or
infection, particularly by
Rubella
virus, as a risk factor that
may precipitate aortic hypoplasia. Acquired MAS is associated
with neurofibromatosis, William’s syndrome, Alagille syndrome,
fibromuscular dysplasia, retroperitoneal fibrosis (Ormond
disease), mucopolysaccharidosis, foetal alcohol syndrome and
Takayasu arteritis.
1-4
In our case, MAS was most likely acquired and caused
by chronic inflammatory disease. The poorly controlled
hypertension diagnosed before surgery was successfully resolved
by the surgery. At the last follow up, the patient did not need any
antihypertensive drugs to control his arterial pressure. Therefore
the duration of malignant hypertension was relatively short and
did not cause any irreversible complications.
On the other hand, severe stenosis of the thoracic and
abdominal aorta is an unusual cause of arterial hypertension
in the upper extremities, independent of the aetiology of
aortic coarctation. Symptoms typically occur within the first
three decades of life and include hypertension, lower extremity
claudication and mesenteric ischaemia. Therefore symptomatic
MAS should be considered a life-threatening condition (possible
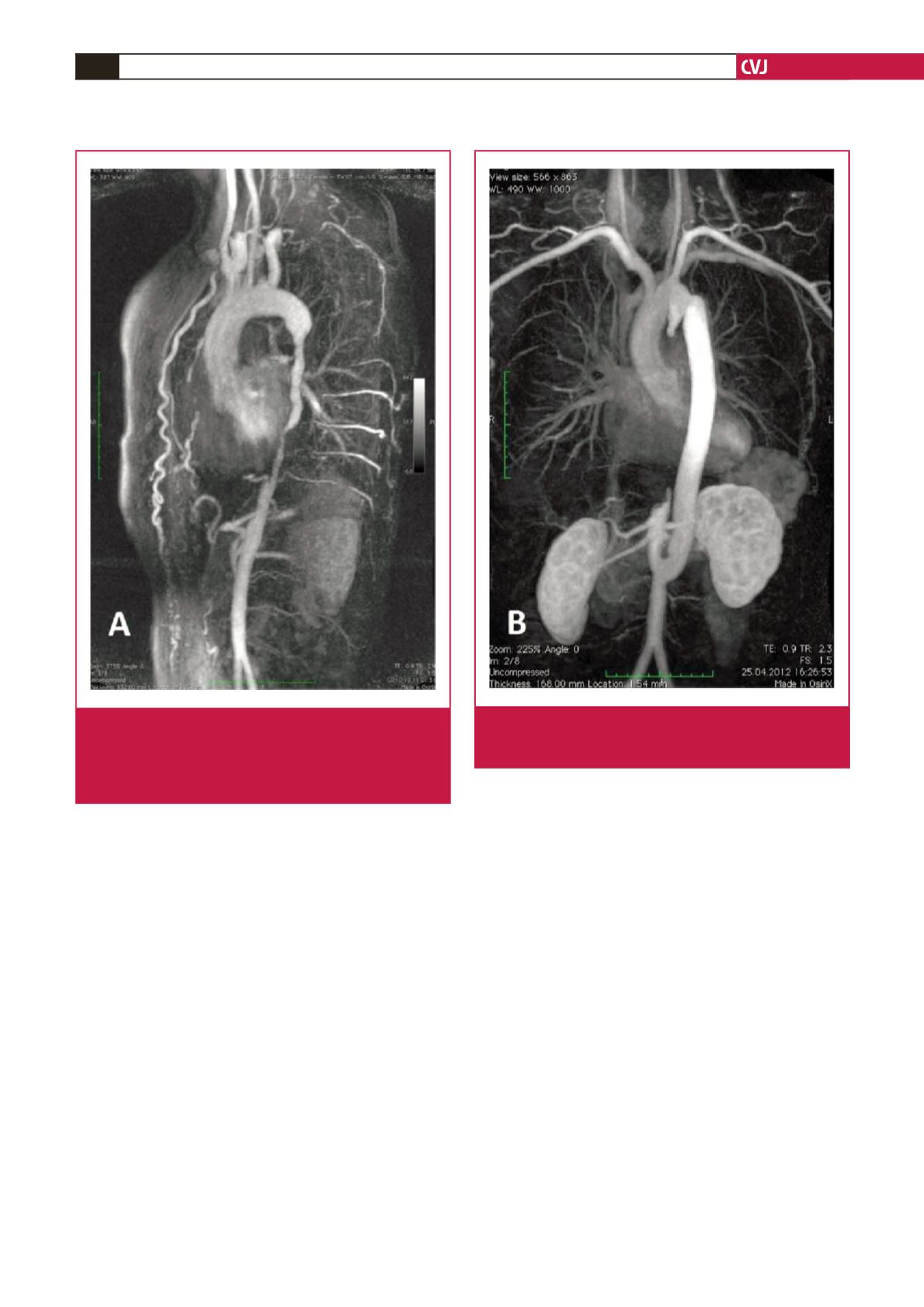
Fig. 1.
Pre-operative MRI. The 180-mm-long narrowing of the
descending aorta with a critical (3–4 mm) coarcta-
tion. The excessively developed collateral circulation,
mainly through intercostal branches and dilated left
and right mammary arteries.
Fig. 2.
Postoperative MRI of the aorto-aortic bypass showing
a patent graft accompanied by a completely occluded
native descending aorta.