
















 29 / 88
29 / 88

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 28, No 4, July/August 2017
AFRICA
231
was compared with 7 563 studies from 296 laboratories in 59
countries around the world.
Patient demographics, clinical characteristics and radiation
dose information for the African and non-African study cohorts
are presented in Table 2. African patients were younger compared
to patients from the rest of the world (60.2
±
11.0 vs 64.3
±
12.0
years;
p
<
0.0001). Median and mean patient ED were similar
in both populations. However, a larger proportion of African
patients received an ED ≤ 9 mSv (49.7 vs 38.2%,
p
<
0.001).
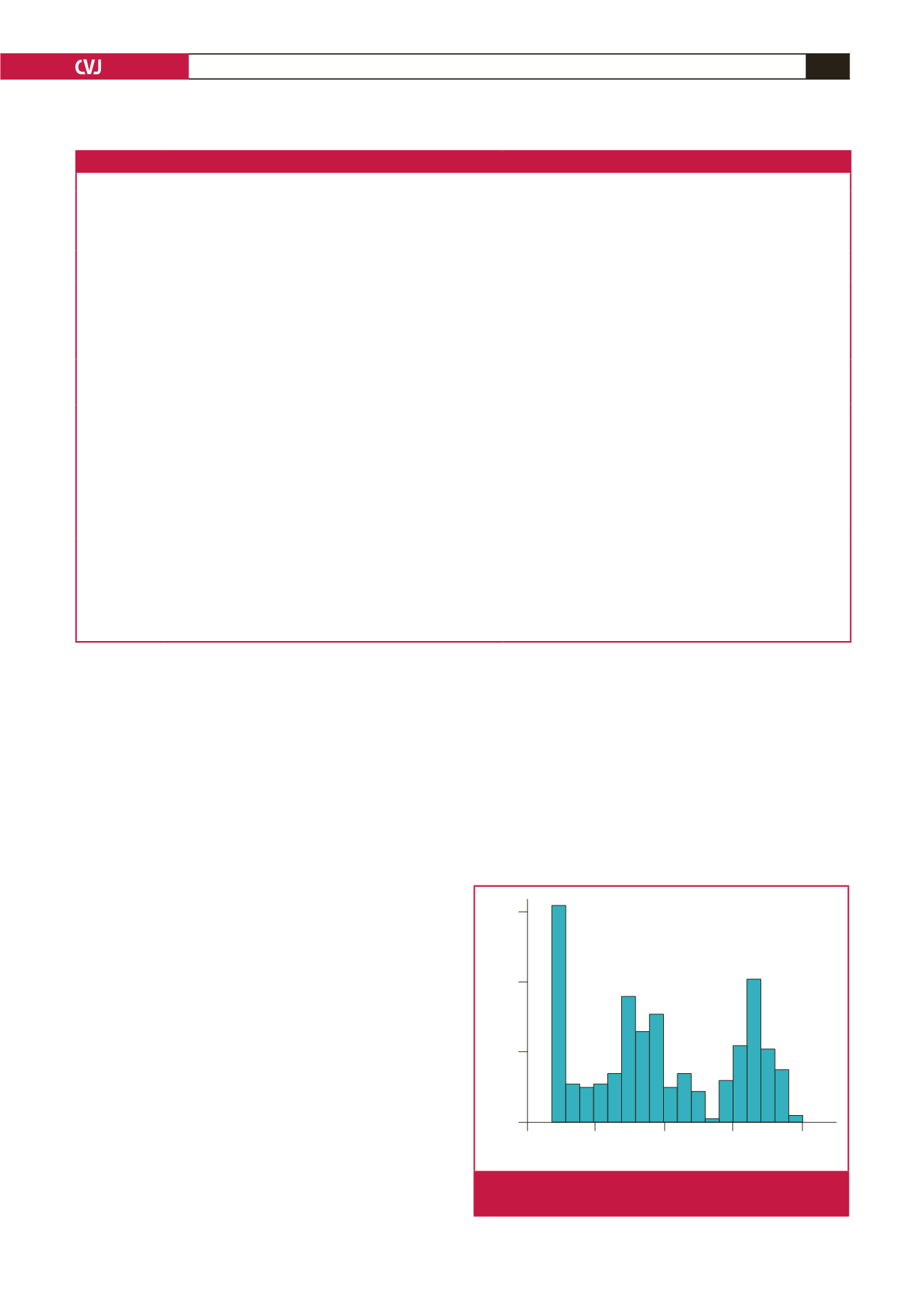
The distribution of individual African patient EDs is presented
in Fig. 1. African patients were more likely than non-Africans to
undergo an MPI study using a stress-only protocol [odds ratio
(OR): 3.4, 95% CI: 2.7–4.3,
p
<
0.001]. The use of PET imaging
was lower in African patients (1.7 vs 6.1%,
p
<
0.0001).
Patient volumes were similar for participating African and
non-African laboratories, as were the laboratory mean and
median ED and the proportion of laboratories with a median
ED ≤ 9 mSv (Table 2). However, there was significant variation
in the ED among African laboratories (median ED range: 2–16.3
mSv,
p
<
0.0001). African laboratory volumes and EDs are
presented in Table 3.
The overall adherence to best practices to minimise radiation
exposure was higher among African laboratories, as reflected
in the mean QI score (6.3
±
1.2 vs. 5.4
±
1.3,
p
=
0.013) and the
proportion of laboratories with a QI score ≥ 6 (75.0 vs 44.9%,
p
=
0.041). However, while the adherence to each individual
best practice was also higher among African laboratories,
this difference failed to reach statistical significance (Table 4).
The only exception was the use of stress-only imaging, which
was used in 66.7% of African laboratories and only 28.7% of
non-African laboratories (
p
=
0.005). The practices of weight-
based dosing and ensuring sufficient administered activity to
avoid shine through were both higher in African laboratories but
failed to reach statistical significance.
Discussion
Africa is facing difficulties in developing nuclear medicine in
general,
14
and the continent has the lowest ratio of clinical
nuclear medicine applications per capita. Few studies
15,16
explicitly
examine nuclear cardiology practice in Africa. The INCAPS
worldwide cross-sectional study of MPI provides a valuable
Table 1. Scoring and explanations of the eight best practices. Adapted from Einstein
et al
.
9
Best practice Scoring
Explanation
Avoid thallium
stress
One point if no thallium-201 studies were performed in
patients
≤
70 years old
SPECT imaging with thallium is associated with a considerably
higher radiation dose to patients compared with technetium-based
radiopharmaceuticals. This item excludes thallium viability studies
and stress redistribution–re-injection stress and viability studies
Avoid dual
isotope
One point if no dual isotope (rest thallium and stress techne-
tium) studies were performed in patients
≤
70 years old
Dual isotope imaging is associated with the highest radiation
dose of any protocol
Avoid
too much
technetium
One point if (1) no study was performed with technetium activ-
ities > 1 332 MBq (36 mCi), and (2) mean total effective dose
was
<
15 mSv for all studies with two technetium injections
1 332 MBq is the highest recommended activity in guidelines,
and 15 mSv is a very high radiation dose for a 99mTc study
Avoid too
much thallium
One point if for each study with thallium, less than 129.5 MBq
was administered at stress
The expert committee maintained that 129.5 MBq should be the
upper threshold for thallium activity
Perform stress-
only imaging
One point if the laboratory performed at least one stress-only
study, in which rest imaging was omitted, or if the laboratory
did only PET-based stress tests
If stress images are completely normal, subsequent rest imaging
can be omitted
Use camera-
based dose-
reduction
strategies
One point if the laboratory performed at least one study using
at least one of the following: (1) attenuation correction (CT or
transmission source), (2) imaging patients in multiple positions,
e.g. both supine and prone, (3) high-technology software (e.g.
resolution recovery and noise reduction), and (4) high-technol-
ogy hardware (e.g. PET or a solid-state CZT SPECT camera)
Each of these approaches reduces the administered activity
needed and facilitates performance of stress-only imaging
Weight-based
dosing for
technetium
One point if the laboratory had a statistically significant posi-
tive correlation between patient weight and administered activ-
ity (MBq), for injections of technetium
Tailoring the administered activity to the patient weight offers an
opportunity to reduce radiation dose
Avoid
inappropriate
dosing that
can lead to
‘shine-through’
artifact
One point if the laboratory performed no SPECT studies with
technetium rest and stress injections on the same day, in which
the activity of the second injection was less than three times
that of the first injection
Shine through occurs in one-day technetium studies when residu-
al radioactivity from the first injection interferes with the images
for the second injection. To avoid shine through, guidelines
recommend that the activity for the second injection should be
three to four times higher than the first injection. A second injec-
tion of less than three times of the activity of the first injection
constituted a dosing that can lead to shine through
Effective dose (mSv)
0
5
10
15
20
Number of patients
60
40
20
0
Fig. 1.
Distribution of radiation-effective dose among observed
African patients.