
















 67 / 88
67 / 88

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 28, No 4, July/August 2017
AFRICA
269
The second version of the roadmap draft was submitted to a
core group for internal review from October to December 2015.
In March 2016, a selected group of hypertension experts from
12 French-speaking countries met in Yaoundé to discuss the
algorithm and the draft.
15
Comments were received and the draft
was amended.
The task force reviewed the final draft of the roadmap in
Mexico in June 2016, which was then submitted for external
peer-review by three independent experts in hypertension and
policy development. The subsequent review was done by a group
of experts in cardiology, nephrology, primary care and research
(including clinical trials). Comments were reviewed and discussed
by the panel and incorporated into a revised and final document.
PASCAR searches and surveys on the status of
hypertension policy programmes and clinical
practice guidelines
From May to July 2015, an internal PASCAR survey was
conducted, aiming to determine which African countries ran
hypertension control programmes focusing on policy. Using the
Survey Monkey software tool,
16
national hypertension experts
from 40 countries were asked whether a hypertension policy
programme was operating in their country and could be judged as
being ‘dormant’, ‘not much active’, ‘active’, or ‘very much active’.
Among the responders (
n
=
127) representing 27 SSAcountries,
we noticed that up to 63.7% did not have a hypertension policy
programme or that it was dormant or not very active. This
regrettable situation highlights the importance of a continental
initiative to develop a hypertension policy to address BP control
from a population-wide and high-risk approach.
Evidence has shown that explicit clinical practice guidelines
(CPGs) do improve the care gap by providing practitioners and
health-service users with synthesised quality evidence regarding
decision-making.
17
In another PASCAR study, we assessed
the existence, development and use of national guidelines for
the detection and management of hypertension in the African
region, regardless of quality.
Between May and July 2015, CPGs for hypertension were
searched, using a scientifically developed search strategy.
Searches were done using Google and PubMed. Search terms
included (country name) AND (hypertension OR HTN OR
high blood pressure) AND (clinical practice guidelines OR
treatment guide). French, Portuguese and Spanish translations
were included in the search strategy.
Websites of ministries of health, national medical associations
and the WHO were hand-searched, authors were e-mailed, and
requests were sent on Afronets to obtain copies of CPGs for
hypertension. To be included in the search, the CPGs had to be
available and provided in full-text versions for assessment by the
review team, comprising three independent authors. CPGs from
Europe or South America or those that could not be obtained
were considered non-existent. Two national hypertension experts
were contacted for confirmation on countries for which we
could not find CPGs on hypertension. CPGs published in peer-
reviewed journals needed to be readily accessed by end-users.
E-mail messages were used for further clarification.
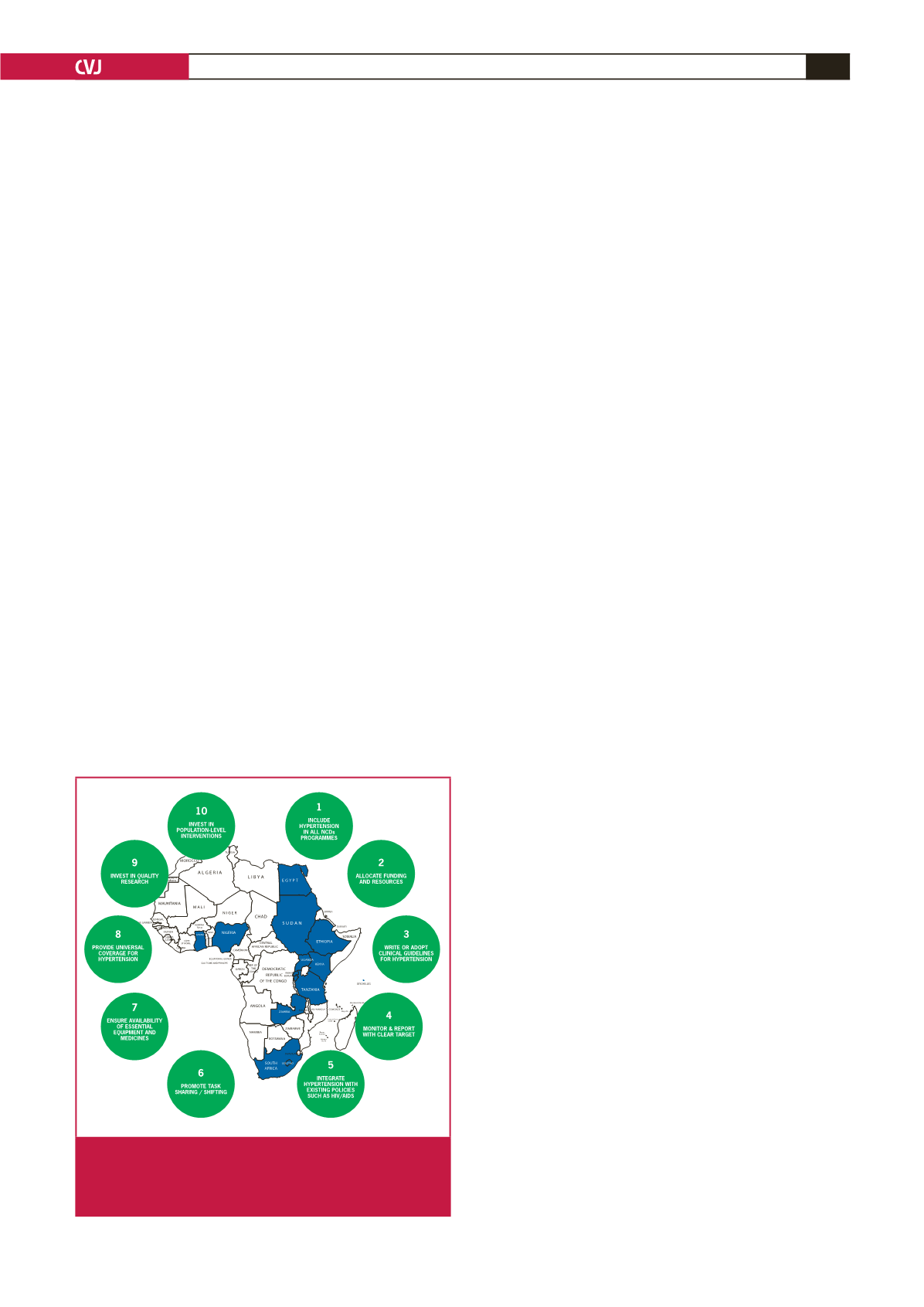
In Fig. 4, the 2015 map is presented of countries with clear
evidence of the existence of national guidelines for detection
and management of BP across Africa. Only 16 (25.8%) out of
62 countries had CPGs complying with our search criteria. No
evidence of CPGs on hypertension management could be found
for the other 46 (74.2%) countries. Given that the only existing
multinational expert recommendations for the management of
hypertension in Africa dates back to 2003 and has not been
updated since,
18
we concluded that there is a legitimate, pressing
need to support African ministries of health with a clear
hypertension roadmap.
PASCAR roadmap to decrease the burden of
hypertension in Africa
To reduce the incidence of CVD through treating hypertension
in the African region, it will be necessary to increase the rates of
detection, treatment and control of the disease. The 10 actions
that need to be undertaken by African ministries of health to
achieve a 25% control of hypertension in Africa by 2025 (Fig. 4)
are listed below and we include an explanation as to why (bullets)
and how (dashes) this needs to be done.
1. All NCD national programmes should additionally contain
a plan for the detection of hypertension.
•
The hypertension crisis has yet to receive an appropriate
response in SSA.
19
•
Incidence of hypertension increased by 67% since 1990
and was estimated to cause more than 500 000 deaths and
10 million years of life lost in 2010 in SSA.
20,21
•
Hypertension is the main cause of stroke, heart failure and
renal disease in SSA.
•
Stroke, which is a major complication of uncontrolled
hypertension, has increased to 46% since 1990 and essen-
tially affects breadwinners.
20
•
Failure to control hypertension and its economic repercus-
sions through revising health policies and services endan-
gers the economic prosperity of all African nations.
22
Fig 4.
2015 map of African countries with evidence of existing
clinical practice guidelines for hypertension manage-
ment and 10 actions to reduce the hypertension
burden in Africa