
















 76 / 88
76 / 88

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 28, No 4, July/August 2017
e2
AFRICA
the aorta–right atrial tunnel. Anterograde cardioplegia was a less
viable option while the shunt between the left and right side of
the heart was still patent. The tunnel was approached and excised
from both ends (Fig. 7), and it was closed directly with bovine
pericardium and prolene sutures at the proximal aorta and right
atrium. The aortic annulus was not damaged during the surgery
and no valvuloplasty was necessary.
There was a large saccular aneurysm in the right atrium. This
was excised and the opening of the windsock was closed directly
with sutures. There was no ventricular septal defect. The right
coronary artery arose from the tunnel and
had atherosclerosis
around its origin, and when opened, the middle portion was also
atherosclerotic. The right saphena magna vein was harvested for the
bypass of the right coronary artery. It was not possible to re-implant
the native right coronary osteum as it was too far removed from the
ascending aorta. Therefore a distal end-to-side anastomosis was
created between the graft and the right coronary artery.
The patient followed up with the cardiologist four weeks
after surgery. All had gone well, and he reported no dizziness
or dysrhythmia. The transthoracic echocardiogram was normal.
Discussion
Aorta–right atrial tunnel is an abnormal extra-cardiac vascular
tunnel between any of the aortic sinuses and the right atrium.
3
The differential diagnosis
includes ruptured aneurysm of the
sinus of Valsalva, coronary arteriovenous fistula, rupture of a
dissecting aneurysm of the ascending aorta into the right atrium,
and pseudo-aneurysm of the right coronary artery followed by
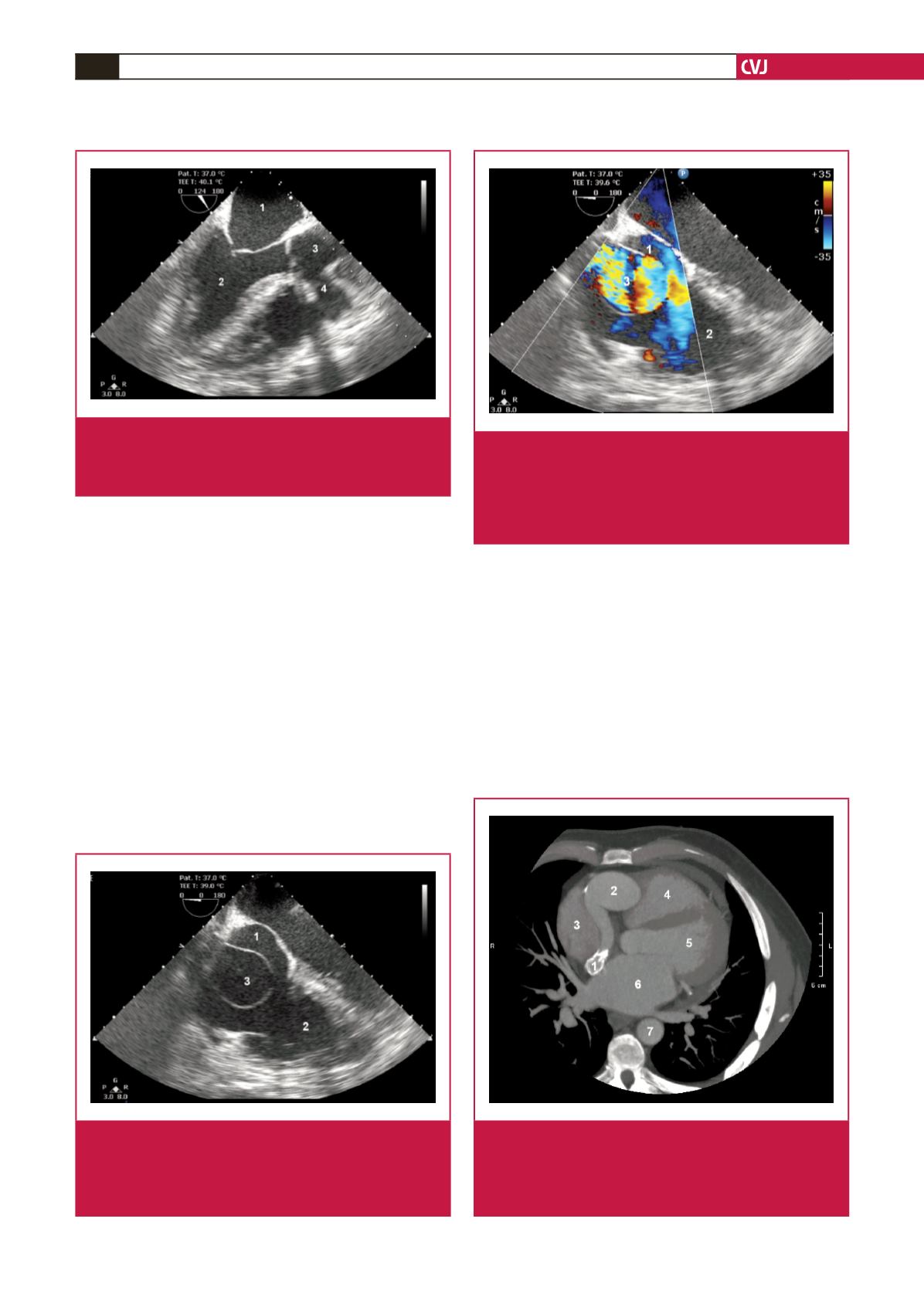
Fig. 1.
Two-dimensional transoesophageal echocardiogram in
long-axis view. 1, left atrium; 2, left ventricle; 3, aorta;
4, origin of tunnel. The origin of the tunnel arises from
the proximal ascending aorta.
Fig. 2.
Two-dimensional transoesophageal echocardiogram
in short-axis view. 1, right atrium; 2, right ventricle; 3,
aneurysmal sac. The windsock arises from the termi-
nal part of the tunnel and is demonstrated within the
right atrium.
Fig. 3.
Two-dimensional transoesophageal echocardiogram
with Doppler in short-axis view. 1, right atrium; 2, right
ventricle; 3, aneurysmal sac. Turbulent flow is demon-
strated within the aneurysmal sac, which empties into
the right atrium through a defect in the wall of the sac,
thus creating the left-to-right shunt.
Fig. 4.
CT angiogram axial image at the level of the left
atrium. 1, distal end of the tunnel; 2, proximal end of
tunnel; 3, right atrium; 4, right ventricle; 5, left ventri-
cle; 6, left atrium. The tunnel is tortuous and dilated.
Distally there are mural calcifications in the tunnel.
1