
















 21 / 74
21 / 74

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 28, No 5, September/October 2017
AFRICA
295
lasted for three months. Most of the junior residents who were
committed to undertaking a career in CTS underwent rotation
in CTS in medical school and as junior surgical residents. The
relationship between the different categories with regard to
interest in CTS and rotation in CTS in medical school was
however not statistically significant (
p
=
0.17), whereas that
between the different categories and posting in CTS during junior
surgical residency was statistically significant (
p
=
0.01) (Table 2).
In most instances, the cardiothoracic surgeons took an interest
in the respondents during their posting. Amajor thoracic procedure
had been observed by 50% (
n
=
119) of junior surgical residents,
while only 13.4% (
n
=
32) had observed an open-heart surgical
procedure. Only 28.2% (
n
=
67) and 2.1% (
n
=
5) had assisted in
major thoracic procedures and open heart surgery, respectively.
Assessment of factors that influence decision of
speciality choice
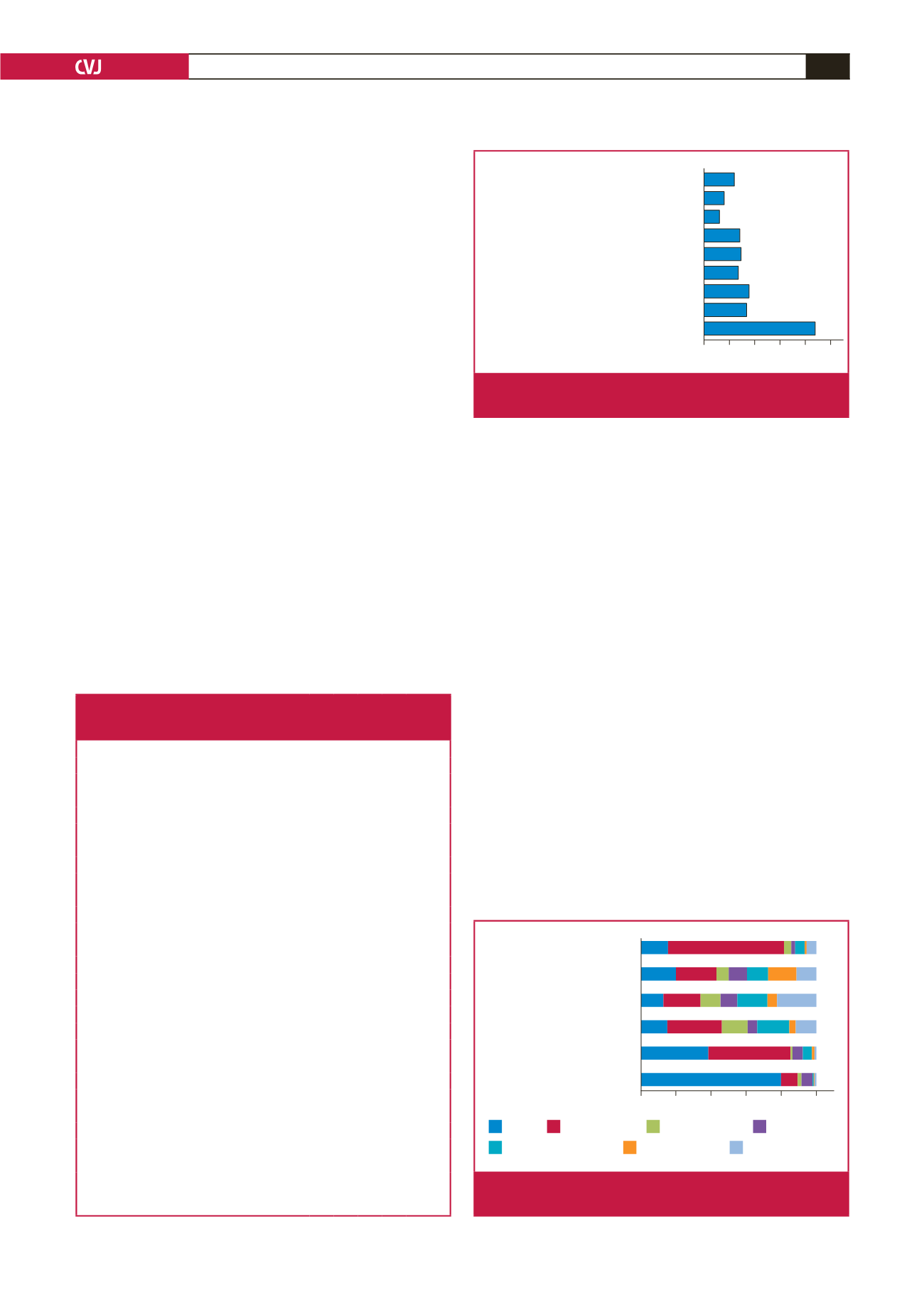
Two hundred and nineteen respondents (92%) identified the type
of procedure and the techniques involved in a speciality as the
most significant factor considered in choice of surgical speciality.
This was followed closely by job opportunities, which was
identified by 89 respondents. Eighty-four respondents (35.3%)
identified the opportunity to engage in a more financially
rewarding practice as the third most popular factor (Fig. 1). The
length of training and advice from colleagues were not popular
factors.
The relationship between all factors considered in the decision
of speciality choice and the different categories of interest in CTS
among junior surgical residents in Nigeria were all statistically
significant (
p
<
0.05). This is an indication that the variations
across the categories of interest in CTS were not by chance.
The respondents were asked about the most important
shortcomings encountered in the practice of the following seven
different surgical specialities (CTS, neurosurgery, plastic surgery,
orthopaedics, general surgery, urology and paediatric surgery).
One hundred and seventy-three respondents (72.7%) believed
that the speciality with the greatest challenge with equipment
was CTS. CTS was identified by 84 respondents (35.3%) to
be second to neurosurgery in having the greatest challenge
with training. Neurosurgery was believed to have the greatest
shortcomings with regard to job dissatisfaction, unfriendly
working atmosphere and being the most time consuming
(Fig. 2).
Factors affecting interest in CTS
Most of the respondents believed the most important factors that
reduce the interest of junior residents in CTS were unavailability
or lack of equipment to function as a cardiothoracic surgeon
(91.2%), limited training positions (64.7%), poor or lack of
exposure in CTS in medical school (58.8%) and poor or lack
of exposure in CTS as junior surgical residents (63%) (Fig.
3). Among those who considered CTS but would specialise
Table 2.The relationship between the four categories of interest in CTS
with age, marital status, level of training, most exciting sub-speciality,
and CTS rotation in medical school and as junior residents
A B C D
p
-value
Age (years)
0.367
26–30
2 16 27 14
31–35
13 38 53 33
36–40
4 13 11 7
41–45
1 1 1 4
Marital status
0.361
Single
9 28 45 26
Married
10 36 47 31
Level of training
0.001
PGY-1
3 23 10 4
PGY-2
10 33 51 25
PGY-3
3 7 20 18
PGY
>
3
4 5 11 11
Most exciting sub-speciality
0.001
Adult cardiac
5 23 20 4
Paediatric cardiac
13 27 36 12
General thoracic
1 15 23 9
Other CT sub-specialities
1 3 4 –
Not excited by any sub-speciality
– – 9 33
Have undertaken CT rotation as a junior resident
0.007
Yes
13 23 30 13
No
7 45 62 45
Undertook CT posting in medical school
0.176
Yes
13 33 36 28
No
7 35 56 30
A: committed to CTS; B: not yet chosen a speciality but interested in CTS; C:
considered CTS but will choose another speciality; D: will neither choose nor
interested in CTS.
0 50 100 150 200 250
One that allows time for family
Length of training
Advice from colleagues
Exposure to positive role model in the speciality
Research opportunity
Opportunity to teach in a medical school
Job opportunities
Opportunity to do a more financially ...
Types of procedure/techniques involved
Fig. 1.
Graph showing factors considered most important in
decision of surgical speciality choice.
0% 20% 40% 60% 80% 100%
Time consuming
Unfriendly working atmosphere
Income
Job dissatisfaction
Challenge with training
Challenge with equipment
CTS
Neurosurgery
Plastic surgery
Orthopaedics
General surgery
Urology
Paediatric surgery
Fig. 2.
Graph showing shortcomings observed with the prac-
tice in different surgical specialties.