
















 68 / 74
68 / 74

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 28, No 5, September/October 2017
e2
AFRICA
She was rehydrated and recommenced on aspirin tablets, while
vascular ultrasound of both legs showed a deep focal vein clot in
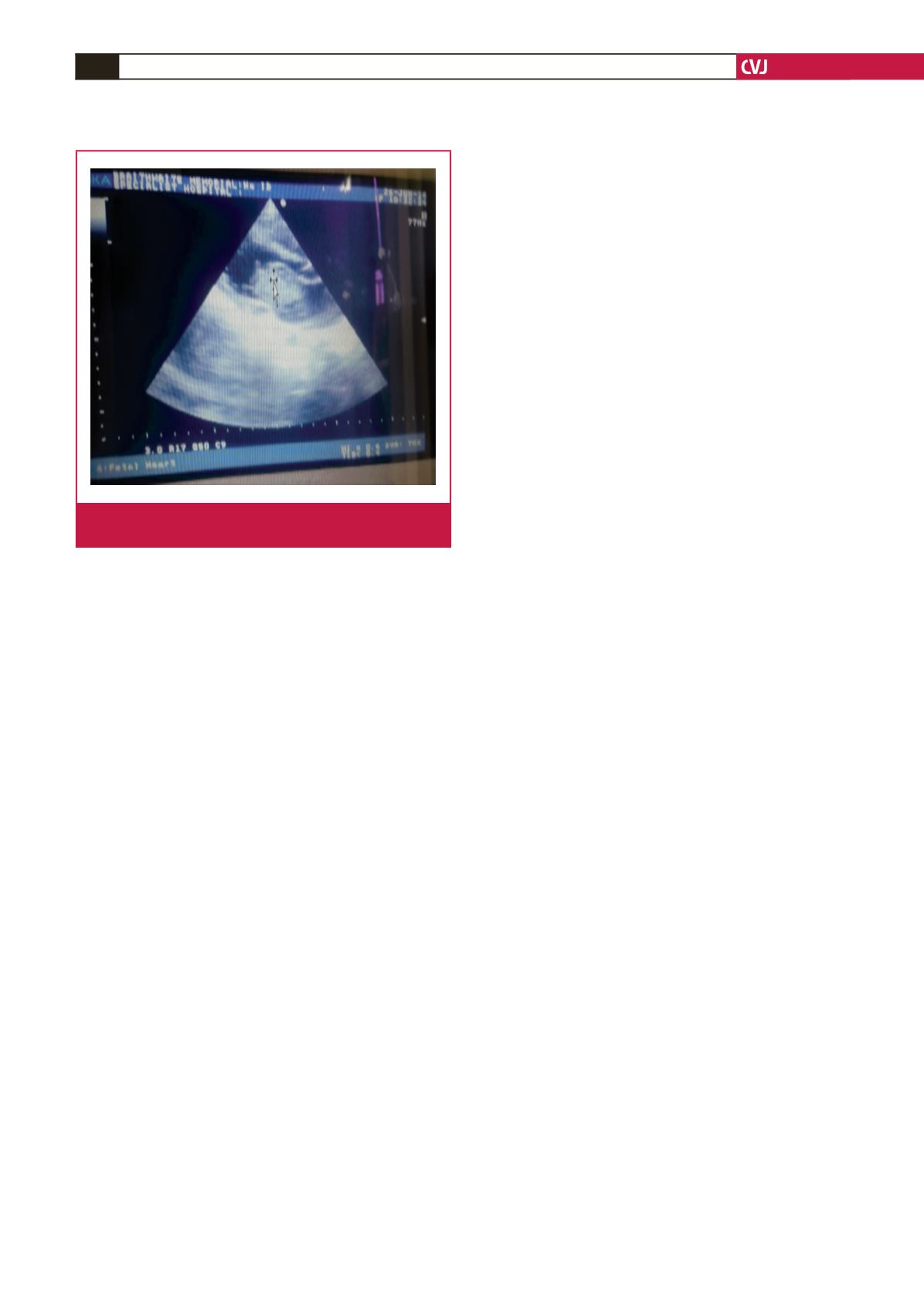
the right common iliac vein. A transthoracic echocardiography
was finally done and it revealed a mobile mass in the left atrium
(myxoma) measuring 3.9 × 2.6 cm impinging on the mitral valve,
a dilated left atrium and multiple ectopic beats (Fig. 1).
A diagnosis of left atrial myxoma with intermittent
arrhythmia and multiple thromboembolic events was made.
Anticoagulation was commenced with heparin and warfarin
tablets. She was also referred for surgical resection of the atrial
myxoma. Due to financial constraints, surgery could not be
done and she died 10 months later while awaiting resection of
the cardiac tumour.
Discussion
Cardiac myxoma accounts for 30% of all primary cardiac
tumours, with a male-to-female ratio of 2:7.
6
The mean age
of presentation is 56 years for sporadic cases and 25 years for
familial cases.
3,7
It is very rarely reported in children; about
three case have been reported in Nigerian children.
8,9
A surgical
incidence of 0.5 atrial myxomas per million population per year
was reported in Ireland.
10
Myxomas may be associated with several syndromes,
namely Carney complex (multiple cardiac and extra-cardiac
myxoma, pigmented skin lesions and endocrine hyperactivity),
LAMB complex (lentigenosis, atrial myxoma, mucocutaneous
myxoma and blue nevi), NAME complex (nevi, atrial myxoma,
neurofibromatosis and ephelides-freckles) and a complex with
lentigenosis, myxoid fibroma of the breast, skin myxomas and
nodular adrenal disease.
Single or multiple gene mutations have been implicated
in the aetiology of cardiac myxoma. They are PRKAR1 on
chromosomes 17 and 2p16. Autosomal dominant transmission is
seen in Carney complex. Atrial myxomas usually occur as a single
lesion and rarely as multiple lesions of varying sizes. They may be
pedunculated lesions or freely mobile and able to move through
the AV valves, as in our patient, or sessile with a broad base.
Cardiac myxomas can be asymptomatic in 20% of cases and
present as sudden death in 15% of cases.
11,12
When symptomatic,
symptoms may be due to intra-cardiac obstruction to blood
inflow and outflow. Our patient’s tumour was causing some
obstruction in the mitral valve. Symptoms can also be due to
mechanical interference with cardiac function, leading to signs
of left- or right-sided heart failure, arrhythmias and syncope,
depending on the location. Our patient had syncope and
intermittent arrhythmias, which were captured clinically by the
irregular pulse; unfortunately when her ECG was done she had
converted to normal rhythm.
Patients may also present with symptoms of systemic or
pulmonary embolisation due to fragmentation of the tumour
cells. Our patient had multiple systemic embolic phenomena
affecting the common iliac vein and cerebral vessels. There
may also be constitutional symptoms in 50% of patients due
to overproduction of interleukin 6 by the tumour cells. These
symptoms include fever, weight loss, lightheadedness and
arthralgia.
A review of nine paediatric cases with atrial myxoma shows
that right hemiparesis was the commonest clinical presentation
in the paediatric age group, occurring in eight (89%) of the
children. Other common symptoms documented were red spots
on the limbs (44%), aphasia (44%), lethargy (22%), seizures,
headache, blindness, slurred speech, dizziness and diplopia
(11%).
13
Pridie also described three children with cardiac
myxoma; all had systemic emboli involving the central nervous
system.
14
A full blood count and blood filmmay show normochromic or
hypochromic anaemia. They can also have haemolytic anaemia
due to mechanical destruction of the erythrocytes by the tumour.
Serum interleukin 6 levels may be high and can be used as a
marker of recurrence.
Chest radiography can show abnormal cardiac silhouette,
mimicking mitral stenosis, tumour calcification and pulmonary
oedema. Echocardiography will show an intra-cardiac mass.
Transoesophageal echocardiography has better specificity and
sensitivity compared to transthoracic echocardiography. We
did a transthoracic echocardiograph for our patient. The point
of attachment of the tumour is best visualised by MRI or CT
scanning. Electrocardiography will show left atrial enlargement,
atrial fibrillation, atrial flutter or other conduction disturbances.
Our patient had left atrial enlargement.
Molecular genetic testing for PRKAR1 may be positive.
Histology shows lipidic cells embedded in a vascular myxoid
stroma, polygonal to stellate shaped, with scanty eosinophilic
cytoplasm.
Surgical resection is the treatment of choice; open heart or
endoscopic resection. Drug therapy is used only for complications
such as congestive heart failure or cardiac arrhythmias.
Post-surgery survival is good, however there is an unusual
recurrence risk of 1–3% in sporadic cases and 20% in familial
cases.
3,15
Biannual echocardiograms are useful for early detection
of recurrent tumors post surgery. Relatives of a child with the
familial type of atrial myxoma should undergo echocardiography
for early detection.
Fig. 1.
Intra-atrial mass measuring 3.9 × 2.6 cm impinging on
the mitral valve, and a dilated left atrium.