
















 71 / 74
71 / 74

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 28, No 5, September/October 2017
AFRICA
e5
was forceful and laterally displaced with an associated fourth
heart sound. He had normal secondary sexual characteristics,
and retinal examination revealed markedly reduced arteriolar
diameter and arteriovenous nicking. The urine dipstick was
normal as was an ultrasound of the kidneys, ureters and bladder.
Chest radiography showed a bulky heart shadow and
electrocardiogram confirmed left ventricular hypertrophy with
a Sokolow–Lyon score of 88 mV. Laboratory investigations
confirmed the hypokalaemia and his serum potassium level was
now 2.7 mmol/l, associated with a supressed renin level of 6.0
mIU/l and aldosterone of 48.6 pmol/l (Table 1). Unfortunately,
arterial blood gas analysis was not performed prior to treatment.
Based on this presentation, genetic testing for the locally
prevalent c.1815G
>
A (p.R563Q)
1
Liddle’s syndrome-associated
genetic variant in the
SCNN1B
gene was requested, and his
treatment was intensified to include doxazosin as no amiloride-
containing medications were available at the time. His blood
pressure remained uncontrolled and the c.1815G
>
A (p.R563Q)
variant screen was negative.
Due to his persistent hypokalaemia, hypertension and
supressed renin and aldosterone levels, sequencing of exon 13
of the beta-chain of the epithelial sodium channel was pursued.
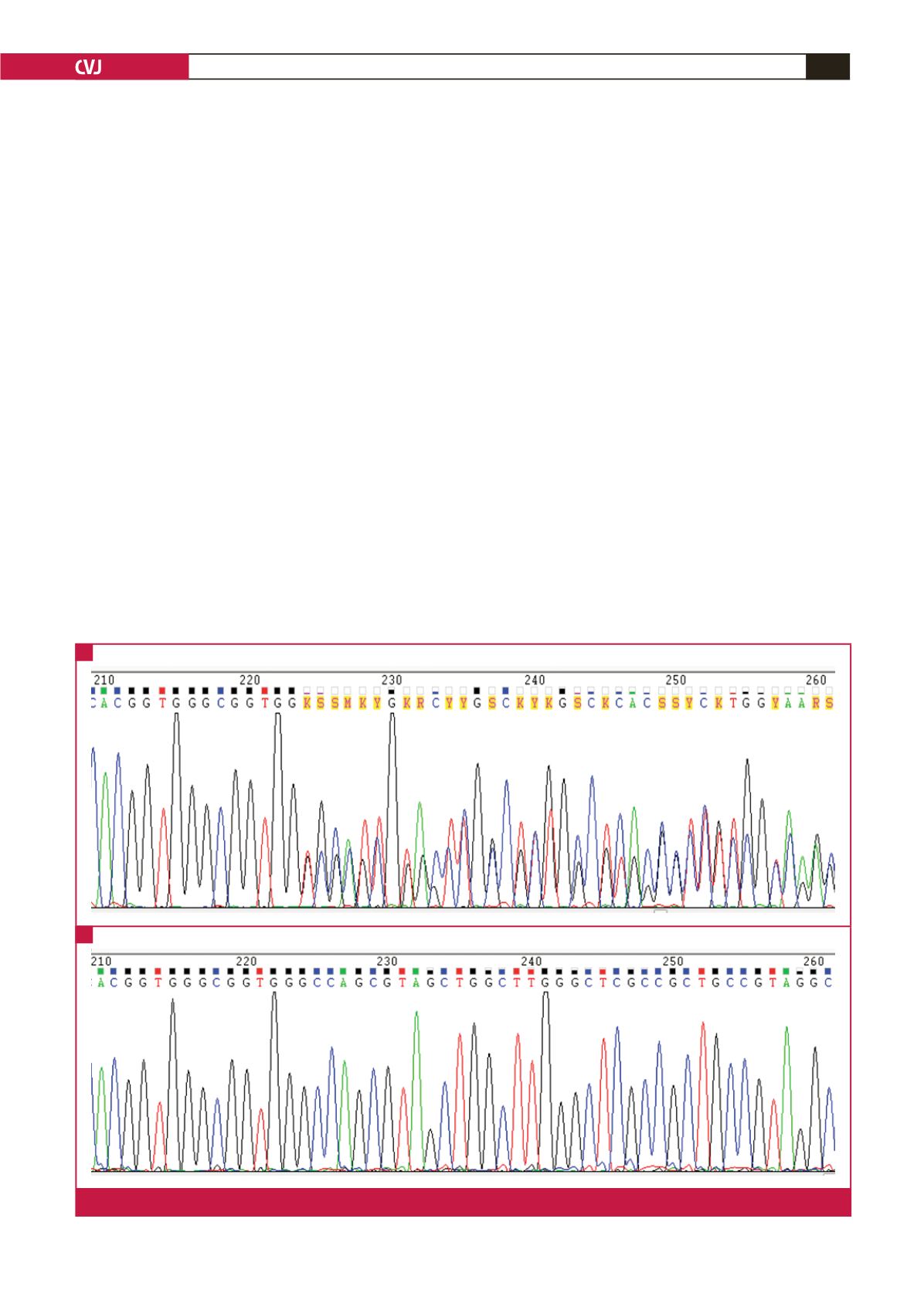
A novel heterozygous 11bp deletion in the
SCNN1B
gene was
detected (Fig. 1A, case and 1B, control). The mutation causes a
frame shift in exon 13 of the gene, resulting in a premature stop
codon and truncated protein product.
His family was called in for screening. We have been unable
to see his mother who lives in a rural area distant from our
clinic. He has two brothers and one sister who are from the same
parents. His younger brother (11 years) and his older sister (21
years) were both well and had normal blood pressures. His older
brother (25 years) was found to have a raised blood pressure of
141/77 mmHg on ambulatory monitoring but was overweight
with signs of insulin resistance and he had a body mass index
of 35.1 kg/m
2
. All three siblings tested negative for the mutation
seen in this patient and had potassium, renin and aldosterone
levels in the normal range.
As amiloride is not registered in South Africa and is only
available in combination with hydrochlorothiazide (5 mg
amiloride; 50 mg hydrochlorothiazide) (Amiloretic, Aspen
Pharmacare, South Africa), he was started on the latter. Over the
next few months his blood pressure improved significantly, with
office readings of 162/91, 139/84, 190/113 and 142/100 mmHg.
He still requires concomitant treatment with enalapril 10 mg
daily, amlodipine 10 mg daily, atenolol 50 mg daily, doxazosin
XL 8 mg daily and potassium replacement. On one occasion,
after running out of tablets for three days, his blood pressure
was 221/157 mmHg.
His creatinine level has remained elevated but he has had no
further headaches. However, potassium levels remain low and we
suspect that higher doses of amiloride are needed. This will be
introduced, pending local regulatory approval.
Fig. 1.
Sequence electropherogram showing the deletion in exon 13 of the
SCNN1B
gene (A), compared to a control sequence (B).
A
B