
















 14 / 74
14 / 74

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 29, No 5, September/October 2018
276
AFRICA
school children. By contrast, in Khartoum the definite-to-
borderline ratio was 0.16:1, in accordance with other studies
done in urban communities.
4,16-18
The definite-to-borderline ratio
in Darfur was much higher than the 1.2:1 that was reported in
Ethiopia.
18
The high RHD prevalence in Darfur is comparable to
that found in Cambodia and South Africa but less than that
found in Ethiopia and Mozambique.
16,18
Similar to our findings,
Engel
et al
. found a disparity between two areas within South
Africa, which was attributed to lower socio-economic status.
18
These findings emphasise the importance of improving medical
services in the most vulnerable rural communities within the
same country and call for effort to be directed to RHD control
programmes in these areas.
It is desirable to have a simplified approach to RHD screening
in remote areas. In this study we documented that the ‘one-view’
protocol decreased screening time, as has been reported by Zühlke
et al
.
11
We have shown that HHE identified 85.2% of cases of
RHD that were detected by SE, with a good agreement between
HHE and SE in diagnosing definite versus borderline RHD.
These findings support the usefulness of HHE in resource-
limited areas in order to improve RHD surveillance, as well as
being a potential mode for early diagnosis and management
of patients in remote, high-risk settings when SE is not
immediately available. Although there is no consensus regarding
the management of echo-diagnosed borderline RHD, there is
preliminary agreement to start prophylaxis for definite cases and
arrange follow-up echo for both definite and borderline cases.
For mitral valve morphological criteria, HHE showed only
a fair agreement with SE. Lu
et al
.
19
reported similar findings
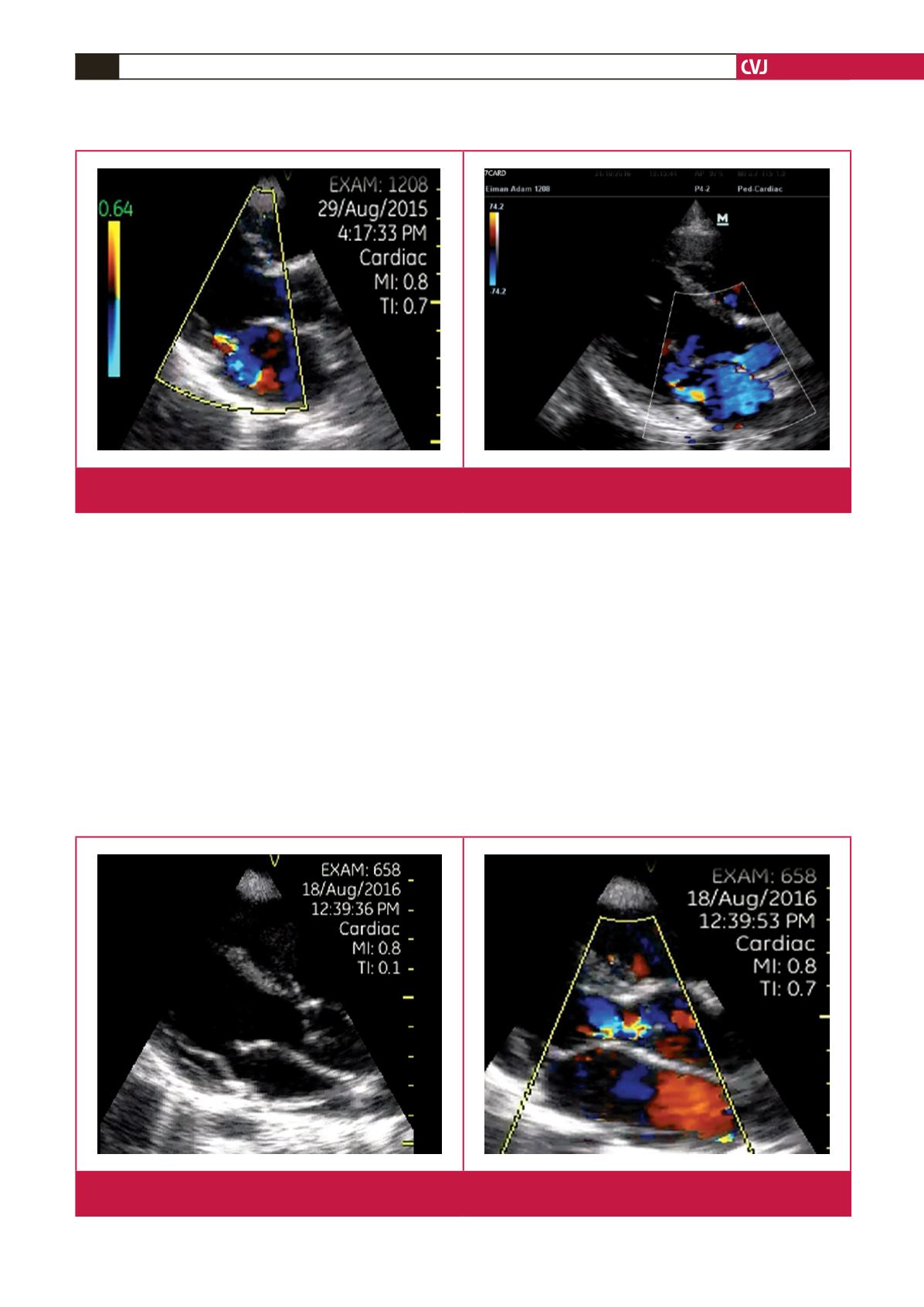
Fig. 3.
A: Hand-held echo in parasternal long-axis view with colour Doppler showing mitral regurgitation. B: Standard echo in
parasternal long-axis view with colour Doppler of the same patient, showing mitral regurgitation.
Fig. 4.
A: Hand-held echo in parasternal long-axis view showing irregularity and prolapse of the aortic valve cusp. B: Hand-held
echo in parasternal long-axis view with colour Doppler for the same patient, showing aortic regurgitation.