
















 41 / 74
41 / 74

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 29, No 5, September/October 2018
AFRICA
303
studies conducted in rural black communities in the Limpopo
province.
3
This may be due to culture-related attitudes, physical
inactivity, poor nutritional value of food, and high intake of
calorie-dense food in rural populations.
3
Obesity is a risk factor for cardiovascular diseases such as
hypertension and type 2 diabetes, and it is a global public health
concern.
13
Van Den Ende
et al
.
9
reported a low prevalence of
overweight and obesity among the same sample at a younger
age (7–15 years). The present study revealed a high prevalence
of obesity (3–26%) and overweight (9–23%) as the ELS sample
grew older. This is a serious concern.
The findings are in line with other studies in Africa and the
prevalence of overweight and obesity continues to increase,
with from 25 to 60% of urban females being overweight.
3,4
The influence of a Western diet together with low levels of
physical activity, particularly among women, as reported by
Sekgala
et al
.,
10
Mchiza
et al
.
6
and Jaffer
et al
.
7
among the South
African population, could be contributing to this escalating high
prevalence of obesity and overweight.
Furthermore, several studies have reported the over-
consumption of macronutrients to be one of the leading causes
of the high prevalence of overweight and obesity among
the adult Saudi population.
19,20
An increase in urbanisation,
in terms of social, political and economic factors, explains
the dietary transition in South Africa among females.
21
It
is projected that the population of overweight and obesity
worldwide will increase to 2.3 billion for overweight and
700 million for obesity.
3
According to the Global Burden of
Metabolic Risk Factors of Chronic Diseases Collaboration
Group, 9.1 million adults are affected with overweight and
obesity.
22
This has caused the tendency of overweight and
obesity to double worldwide.
The intake of carbohydrates and fats in the present study
was higher than that reported by Van Den Ende
et al
.
9
in the
same sample at a younger age. Singh
et al
.
2
recommended 60%
carbohydrate, 30% total fats and 10% protein as the total daily
kilocalories for an individual. The high consumption of fats in
our study therefore reveals that there is a peak in the nutritional
transition, and weight status has therefore changed among Ellisras
females. The high intake of saturated fat reported in this study is
in agreement with that in healthy young adults in Saudi Arabia.
23
The significant association between dietary intake and BMI
predicts that the higher the percentage of kilojoules, the higher
the risk of overweight and obesity. This finding is consistent
with Van Den Ende
et al
.
9
Sengwayo
et al.
3
found a significant
association of dyslipidaemia with high BMI among females
in Limpopo. This is associated with a shift in the nutritional
pattern, which predisposes to the development of atherosclerosis
due to a high cholesterol intake.
A limitation of this study is the cross-sectional design,
which does not allow an analysis of cause and effect regarding
the association between BMI and dietary intake. Also we
did not consider blood sample analysis to support the
findings of dietary intake. However, Steyn
et al
.
21
confirm
that dietary intake can be reliably evaluated by assessing
the macronutrient intake. All anthropometric data were
measured, not self-reported by the participants, which allows
the comparison of our study with other studies in South
Africa to be accurate.
4,21
Furthermore, we used interviewer-
administered questionnaires, which are more effective than a
self-administered questionnaire.
5
Conclusions
There was a high prevalence of overweight and obesity among
rural Ellisras females. Cholesterol intake was associated with a
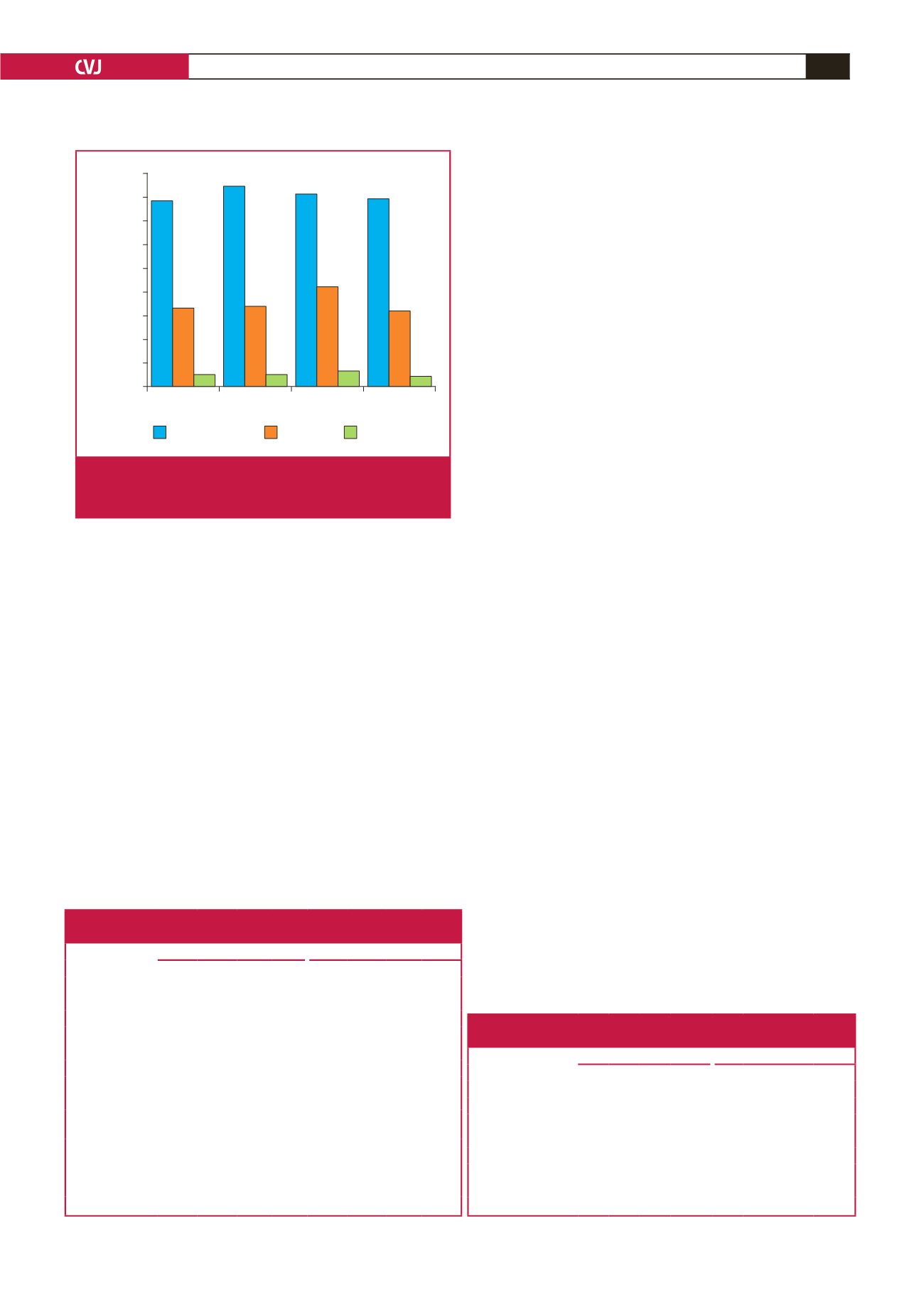
Nutritional status
78.2
84.5
81
79.1
32.8
33.7
42
31.6
4.8
4.7
6
4.1
Underweight
Normal
Overweight
Obese
Macronutrients (%)
90
80
70
60
50
40
30
20
10
0
Carbohydrates
Total fat
Saturated fat
Fig. 3.
Descriptive statistics for 24-hour recall of dietary intake
by nutritional status of young rural Ellisras adults aged
18–30 years.
Table 2. Linear regression coefficient, 95% CI and
p
-value in the
association with body mass index and dietary intake
Unadjusted
Adjusted (age and gender)
BMI variables
β
95% CI
p
-value
β
95% CI
p
-value
Total fat
–0.002 –0.011 0.007 0.665 –0.001 –0.010 0.007 0.738
Animal protein 0.000 –0.016 0.015 0.988 0.004 –0.010 0.018 0.538
Plant protein
–0.001 –0.041 0.038 0.951 0.008 –0.028 0.044 0.667
Total sugar
0.009 –0.010 0.028 0.366 –0.002 –0.019 0.015 0.827
Carbohydrates
0.001 –0.002 0.004 0.545 0.001 –0.002 0.004 0.459
Total dietary fibre 0.016 –0.040 0.073 0.570 0.019 –0.032 0.071 0.460
Total protein
0.000 –0.013 0.014 0.972 0.005 –0.007 0.017 0.451
Cholesterol intake 0.002 0.000 0.004 0.058 0.002 0.000 0.004 0.035*
Mono-unsaturat-
ed fatty acids
–0.008 –0.032 0.016 0.527 –0.005 –0.027 0.016 0.634
Polyunsaturated
fatty acids
–0.002 –0.033 0.028 0.876 –0.002 –0.029 0.026 0.899
Saturated fatty
acids
–0.007 –0.033 0.019 0.600 –0.007 –0.030 0.017 0.583
CI: confidence interval,
β
: beta-coefficient. *Significant at
p
< 0.05.
Table 3. Logistic regression for the association between
overweight/obesity and low dietary intake
Unadjusted
Adjusted for age and gender
Variable
OR 95% Cl
p-value OR 95% CI
p-value
Overweight/obesity
Total fat
0.78 0.56 1.10 0.154 0.86 0.59 1.22 0.430
Total sugar
1.18 0.67 2.08 0.561 0.96 0.52 1.78 0.900
Saturated fat
1.23 0.89 1.69 0.215 1.32 0.924 1.894 0.127
Mono-unsaturated fat 0.61 0.20 1.88 0.388 0.48 0.14 1.694 0.255
Polyunsaturated fat
1.48 0.25 8.93 0.668 1.46 0.20 10.81 0.708
Cholesterol intake
1.43 0.95 2.16 0.084 1.73 1.09 2.75 0.020*
OR: odds ratio; CI: confidence interval. *Significant at
p
< 0.05.